On this page
Psychiatrists face unique social media challenges that no other specialty deals with: extreme patient privacy concerns, content that triggers platform moderation algorithms, stigma that makes patients hesitant to engage publicly, and ethical boundaries that limit what you can share. Despite all this, social media is the most powerful tool psychiatrists have for normalising mental health care and building a practice.
The psychiatrists in our network who've navigated these challenges well have built practices with 3-month waiting lists. Here's exactly how they did it.
Q.Why Should Psychiatrists Be on Social Media Despite the Risks?
Because stigma is the #1 barrier to mental healthcare, and social media is the #1 tool for fighting stigma at scale.
The numbers are clear:
- 56% of people with mental health conditions don't seek treatment, primarily due to stigma
- 78% of adults under 35 who eventually sought psychiatric help said social media content by mental health professionals influenced their decision
- Mental health content on Instagram generates 4x the save rate of general medical content — people save it privately, even if they don't engage publicly
- 1 in 3 new psychiatric patients in our network cite "saw the doctor's social media" as their discovery channel
The psychiatrist who stays off social media doesn't avoid risk — they simply cede the conversation to unqualified influencers, wellness coaches, and misinformation.
Q.What Are the Content Rules Psychiatrists Must Follow?
Platform-Specific Restrictions
Social media platforms have content moderation policies that directly affect mental health content:
| Platform | Key Restrictions | Workarounds |
|---|---|---|
| Flags suicide/self-harm content; may suppress posts with trigger words | Use positive framing ("seeking help" vs "suicidal thoughts"); add "sensitive content" warning slides | |
| YouTube | Demonetises mental health content with graphic descriptions | Focus on recovery narratives and coping strategies; avoid detailed descriptions of methods |
| TikTok | Restricts content about eating disorders, self-harm; age-gates mental health content | Frame content around professional help-seeking; avoid first-person crisis narratives |
| Minimal restrictions but professional context expected | Clinical perspective, research summaries, industry commentary |
Ethical Guidelines
- Never share patient information: Even de-identified cases should be composited (combining elements from multiple patients) to prevent recognition
- Don't diagnose through content: "5 Signs You Might Be Depressed" is acceptable. "If You Have These 5 Signs, You Have Depression" is not
- Include professional help resources: Every post about a serious condition should include helpline numbers or a "consult a professional" message
- Avoid triggering content: Don't describe crisis situations in graphic detail. Focus on recognition and help-seeking, not on the experience itself
- Maintain boundaries: Don't respond to crisis DMs with clinical advice. Have a standard response that directs to emergency resources
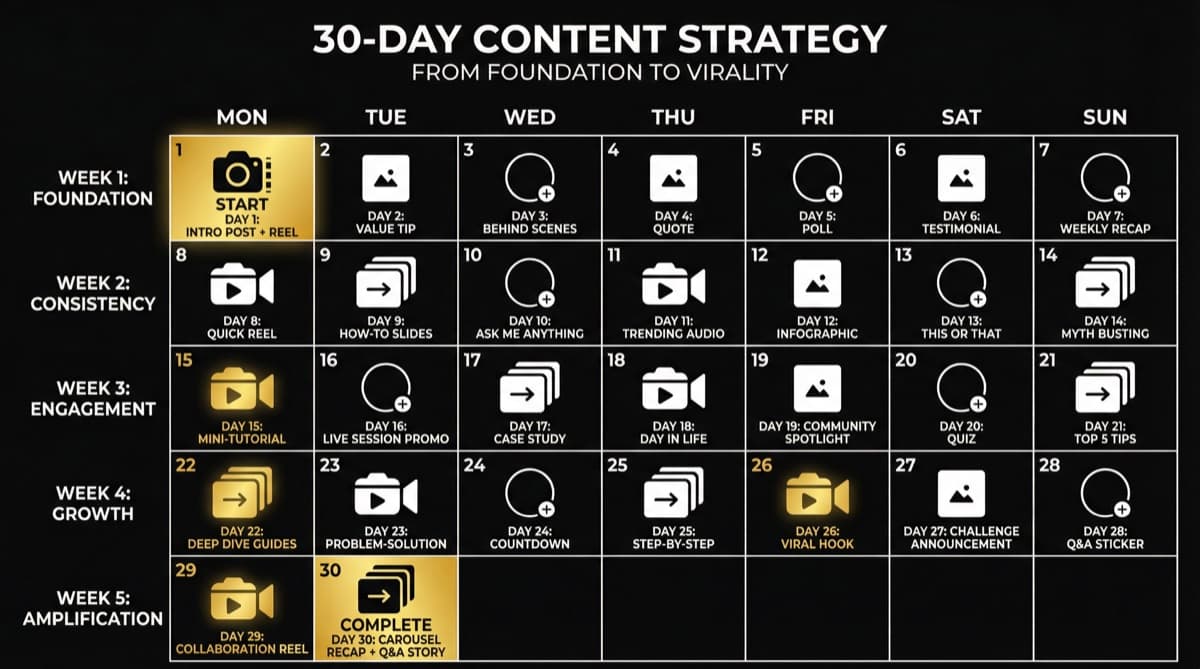
Q.What Content Strategy Works for Psychiatrists?
The Stigma-Reduction Framework
Content should follow a specific hierarchy designed to normalise help-seeking:
Tier 1: Education (40% of content)
- What different conditions actually look like
- How psychiatry works (first appointment walkthrough, what to expect)
- Medication myths vs facts
- "When to see a psychiatrist vs a psychologist vs a counsellor"
Tier 2: Normalisation (30% of content)
- "Things mentally healthy people also experience"
- Workplace mental health discussions
- Relationship and family mental health
- Seasonal mood changes and stress management
Tier 3: Empowerment (20% of content)
- Coping strategies and tools (that complement professional treatment)
- Recovery stories (composited, never identifiable)
- Professional achievement stories of people who sought help
- Self-care frameworks grounded in evidence
Tier 4: Professional Authority (10% of content)
- Your credentials, continuing education, conference appearances
- Published research or case studies
- Media appearances and interviews
- Practice updates and new services
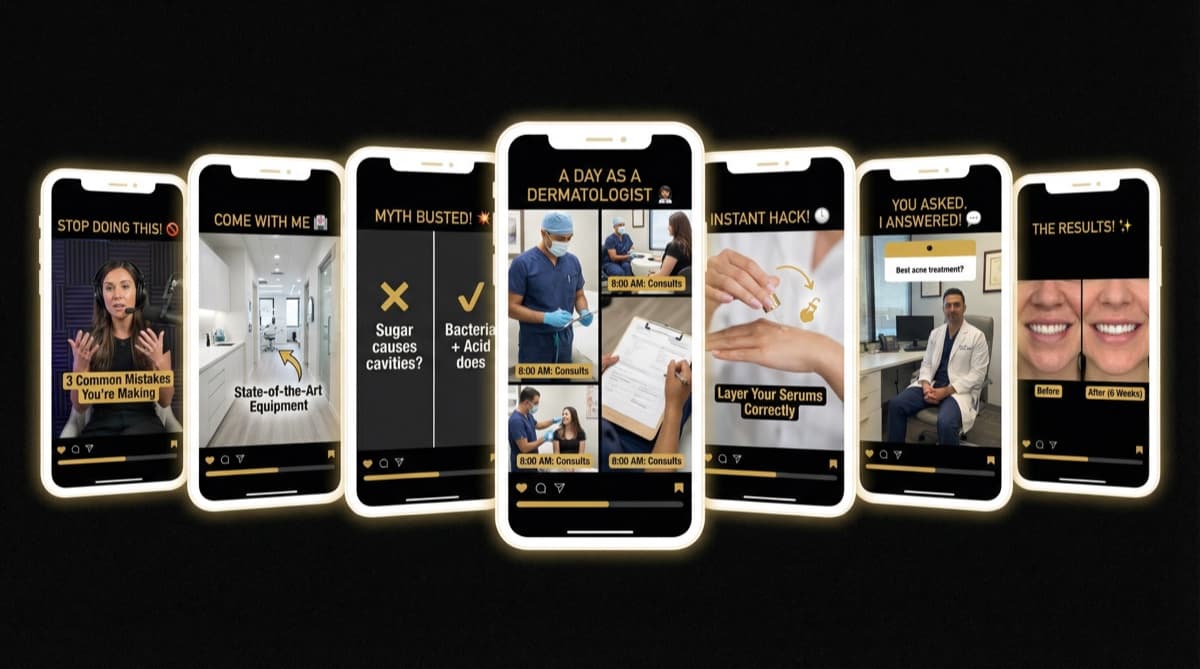
Content Formats That Work Best
- 1Carousels (highest save rate): "7 Things Your Therapist Wants You to Know" — educational, non-triggering, highly saveable
- 2Talking-head Reels (highest trust): You speaking directly to camera about a mental health topic. Keep it 30-60 seconds. No background music — your voice is the trust signal
- 3Text-based posts (highest share rate): Simple, powerful statements — "Going to therapy doesn't mean you're broken. It means you're building." These get shared privately
- 4Q&A Stories (highest engagement): Weekly "Ask Me Anything" in Stories. Patients ask anonymously, you answer on camera
Need help with this?
Our team specializes in healthcare branding. Get personalized advice in a free 15-minute call.
Book a free 15-minute callQ.How Do You Build Patient Trust Without Violating Privacy?
This is the central tension in psychiatric social media. Here's how to navigate it:
Never:
- Share patient stories — even "fully de-identified" ones can be recognised by the patient or their family
- Respond to DMs with clinical advice
- Confirm or deny that someone is your patient (even if they publicly say so)
- Use patient quotes or testimonials (without explicit written consent — and even then, reconsider)
Instead:
- Share composite cases that combine elements from multiple patients and published literature
- Use hypothetical scenarios: "A person experiencing X might benefit from Y"
- Share your own professional perspective and clinical reasoning
- Reference published research and population data rather than individual cases
- Encourage reviews on Google (where patients choose to share publicly) rather than soliciting testimonials
Q.How Do You Handle Crisis Situations in DMs?
You will receive DMs from people in crisis. This is inevitable for any psychiatrist on social media. Have a protocol:
- 1Saved response for crisis messages: "Thank you for reaching out. If you're in immediate danger, please contact [local emergency number] or [crisis helpline]. I take your wellbeing seriously, and a proper assessment requires a clinical consultation. Would you like to book an appointment?"
- 2Pin emergency resources: Keep crisis helpline numbers in your bio, Story Highlights, and as the first comment on posts about serious conditions
- 3Don't ignore crisis DMs: Acknowledge receipt and direct to appropriate resources. Ignoring a crisis message creates liability risk
- 4Document your responses: Maintain a record of your protocol and responses in case of legal questions
- 5Set business hours: Use Instagram's automated messaging to set expectations: "Thank you for your message. I respond during business hours (9 AM - 6 PM). If this is an emergency, please call [emergency number]"
Q.What Results Can Psychiatrists Expect From Social Media?
Based on data from 12 psychiatrists in our network:
- Months 1-3: Building content library. 500-2,000 followers. 1-3 patient inquiries per week
- Months 4-6: Content gains traction. 2,000-5,000 followers. 5-10 patient inquiries per week
- Months 7-12: Established presence. 5,000-15,000 followers. 10-20 patient inquiries per week
- Year 2+: Authority position. 15,000-50,000 followers. Waiting list of 2-4 weeks for new patients
The financial impact: a psychiatrist charging Rs 1,500-2,500 per session (India) or $200-400 per session (US) who gains 10 new weekly patients from social media adds Rs 60,000-1,00,000 or $8,000-16,000 in monthly revenue.
FAQ
Q:Won't being on social media make me seem unprofessional to colleagues?
A:Five years ago, maybe. In 2026, not being on social media as a mental health professional seems disconnected from where patients are. 78% of adults under 35 use social media as their primary mental health information source. Your colleagues who aren't on social media aren't maintaining professionalism — they're ceding influence to unqualified voices.
Q:How do I handle negative comments from anti-psychiatry advocates?
A:Don't engage in debates. Use a simple, evidence-based response: "I respect different perspectives. The evidence supporting psychiatric treatment for conditions like major depression and anxiety disorders is well-established. I'm here to provide accurate information and help those who want help." Then move on. Block persistent harassers.
Q:Should I share my own mental health experiences on social media?
A:This is deeply personal. Some psychiatrists find that sharing their own experiences with therapy or mental health challenges builds extraordinary trust. Others prefer to maintain professional distance. There's no right answer — but if you choose to share, do so deliberately, not impulsively. Test the content with a trusted colleague before posting.
Q:How do I price my services when patients come through social media?
A:Don't discount. Social media patients are not lower-value — they're often higher-value because they've already built trust with you through your content. Charge your standard consultation fees. If anything, the pre-built trust means they're more likely to commit to treatment plans and refer others.