On this page
India added 60% more medical colleges in the last 10 years (from 382 to 610+). Rural doctor availability didn't improve. Why? Because education policy can't fix market incentive problems. You can graduate a thousand cardiologists, but if rural cardiology pays Rs 3L/year and urban pays Rs 50L, they'll all move to cities. The problem isn't supply — it's distribution. Production does not equal distribution does not equal retention.
The Medical College Expansion Myth
2010: 382 medical colleges, 26,000 seats/year, 5,000 specialty seats. 2015: 445 colleges, 30,000 seats, 8,000 specialty. 2020: 545 colleges, 36,000 seats, 12,000 specialty. 2024: 610+ colleges, 42,000 seats, 16,000 specialty.
Looks like growth. But doctor distribution: Total doctors in practice went from 850,000 (2010) to 1.5M (2024) — +76% (good). Doctors in rural areas went from 180,000 to 280,000 — +56% (but population grew 15%). Doctor:Population ratio (rural) went from 1:4,100 to 1:4,200 — worsened. Percentage of doctors in cities went from 68% to 72% — concentration increased.
More doctors overall. But rural doctor shortage worsened relative to population growth.
Q.What Is The Production-Distribution Gap?
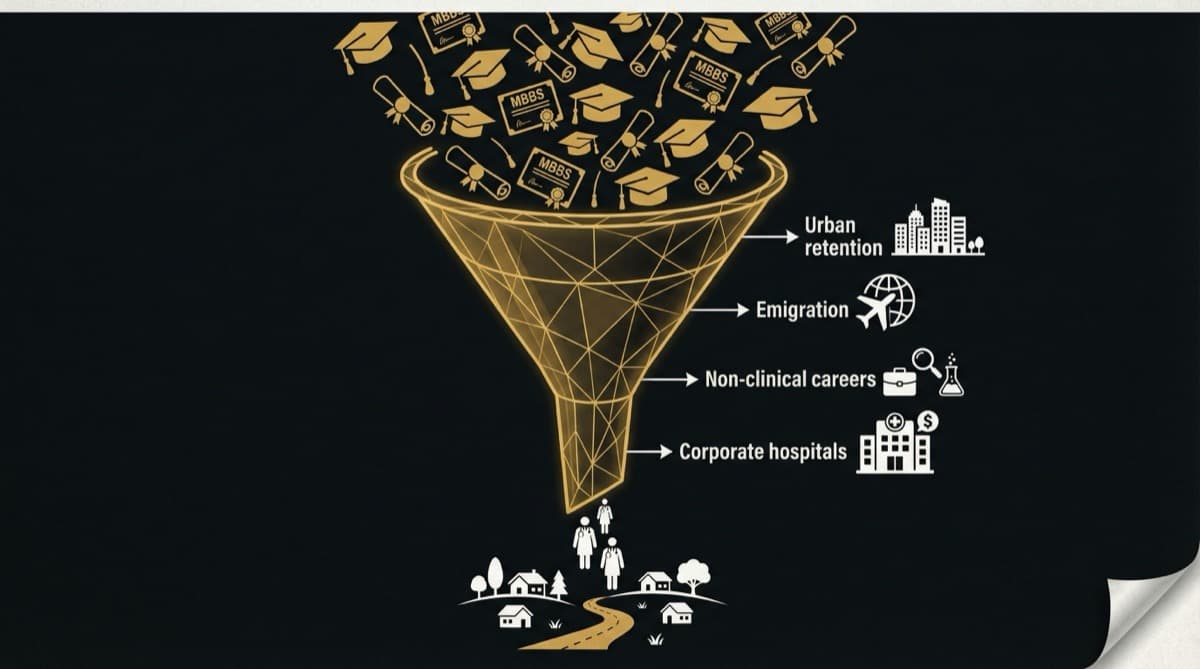
India optimized for Production (training). Ignored Distribution (job choice). Ignored Retention (staying).
Where do fresh graduates choose to practice (5 years post-college)? Metro city 55%. Tier-2 city 25%. Tier-3 town 12%. Rural area (voluntary) 3%. Rural area (government posted) 5% (temporary).
Even with 2,500 rural seats, only 3-5% voluntarily stay in rural areas.
Retention after rural posting: Year 1 95% (mostly government-posted). Year 2 75%. Year 3 45%. Year 5 25%. Year 10 15%.
A doctor trained in rural school and posted rural in Year 1 has an 85% chance of being in a city by Year 10.
Q.Why Education Policy Can't Fix Incentive Problems?
At Year 2 (end of mandatory service), you have a choice: Stay rural (Rs 75K/month, career stagnation, kids' education compromised) or move to metro (Rs 2.3L/month, career growth, kids' education secured). What education policy could convince you to choose option 1? None. Because education doesn't change market incentives.
What education policy did vs what market incentives require: Increased rural training seats vs (needed) higher rural doctor salaries. Improved rural curriculum vs (needed) specialist support in rural areas. Added rural skill training vs (needed) career growth opportunities in rural. Increased enrollment capacity vs (needed) school infrastructure in rural towns.
No overlap. India added rural medical seats. But the market continued rewarding metro practice. Graduates responded rationally by moving to metros.
Q.What Is Rural Doctor Availability Before and After Expansion?
Doctor per 1,000 (rural India): 2010: 0.24. 2024: 0.24. Target (WHO) 1.0. No improvement. Specialist availability (rural): 2010: 2%. 2024: 3%. Target 30%. No improvement.
60% more doctors trained. Zero improvement in rural metrics.
New medical colleges opened mostly in tier-2 cities, not rural areas. 48% of new capacity added in tier-2 cities. Only 6% in rural areas. Graduates from tier-2 colleges migrate to metros within 3-5 years.
Need help with this?
Our team specializes in healthcare branding. Get personalized advice in a free 15-minute call.
Book a free 15-minute callQ.What Would Actually Fix Rural Healthcare?
Raise rural salaries to metro levels: Government budget increase Rs 10,000Cr/year. Build specialist infrastructure in rural: Rs 20,000Cr over 10 years. Improve rural schools/social infrastructure: Rs 30,000Cr over 10 years. Incentivize rural practice (loan forgiveness): Rs 2,000Cr per year.
Medical college expansion cost: Rs 5,000Cr. But it's treating the wrong problem.
If you want rural doctors: Rural salary floor at 80% of metro (current: 30%). Career growth possible in rural. Family support (schools, spouse income, social life). Exit strategy (allow rotation, not permanent posting).
Frequently Asked Questions
Q: Hasn't rural doctor availability improved in absolute numbers?
A: Yes, from 180K to 280K. But rural population grew 15%, so the ratio worsened.
Q: Could we mandate rural service longer (5-10 years)?
A: Doctors would leave medicine. Forced workers are bad workers. Also violates freedom of practice.
Q: Why did government keep adding colleges if it wasn't working?
A: Because "increased seats" is a visible policy success. "Rural doctor distribution still terrible" doesn't fit the narrative. It's bureaucratic success theater, not healthcare problem-solving.
India's medical college expansion is a case study in solving the wrong problem. More doctors, same distribution problem, rural healthcare still failing.
futurise. builds premium healthcare brands in 48 hours. Learn more at futurise.studio