On this page
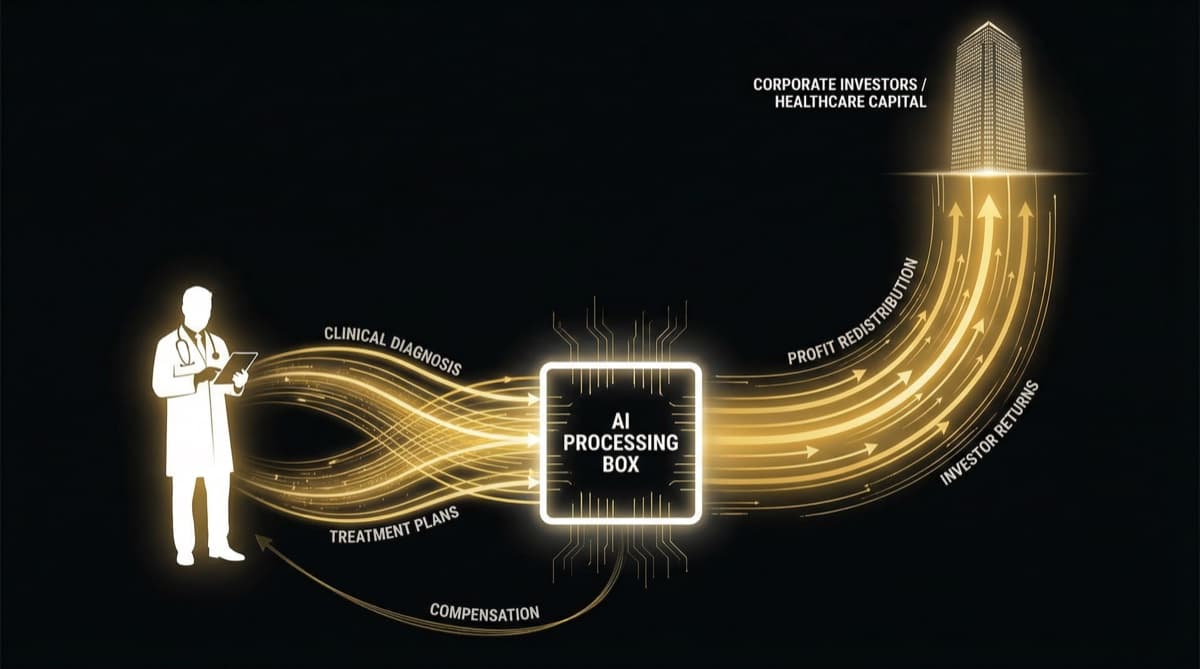
AI in healthcare follows a three-phase pattern that every Indian doctor needs to understand: Phase 1 is panic ("AI will replace us!"), Phase 2 is relief ("AI is just a tool that helps us"), and Phase 3 is the quiet salary cap — where AI-boosted productivity becomes the new baseline, hospitals capture the efficiency gains, and doctor compensation stagnates or declines relative to the value they generate. AI doesn't eliminate doctors. It shifts leverage from the doctor to the hospital. And in India's PE-backed hospital system, where EBITDA optimization already drives compensation decisions, AI is the next structural tool for capturing more clinical output at lower per-unit doctor cost.
The Three-Phase Pattern
Q.What Is Phase 1: Panic (2018-2022)?
Headlines read: "AI Will Replace Radiologists." "Doctors Face Automation Threat." Medical students wondered whether choosing radiology or pathology was career suicide.
The fear was based on real capability demonstrations — AI systems matching or exceeding specialist performance in specific diagnostic tasks. But it fundamentally misunderstood how healthcare labor markets work. Doctors aren't replaced by technology; they're repositioned by it.
Q.What Is Phase 2: Relief (2022-2025)?
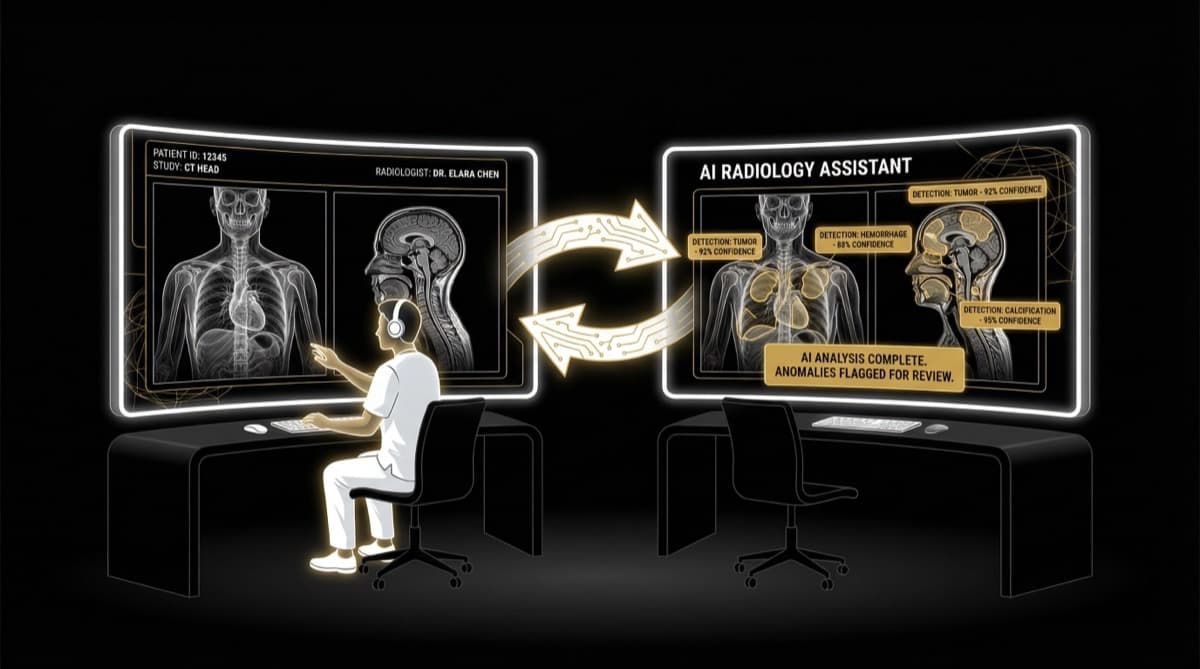
The narrative shifted to: "AI is a tool, not a replacement." Radiologists don't lose jobs — they become more efficient. Pathologists don't get fired — they validate AI reads. The medical profession collectively exhaled.
This phase feels reassuring. And it's technically accurate. But it obscures what's actually happening underneath.
Q.What Is Phase 3: The Quiet Salary Cap (2025-onwards)?
This is the phase most doctors haven't recognized yet. It works like this:
- 1AI enables a radiologist to read 170 studies/day instead of 100
- 2Hospital revenue per radiologist increases by 70%
- 3Radiologist salary: unchanged (or marginally increased)
- 4Hospital captures the productivity differential as EBITDA improvement
- 5New radiologists enter a market where AI-assisted volumes are the expected baseline
- 6The scarcity premium that drove radiology compensation erodes
- 7Outcome: doctors produce more value, capture less of it
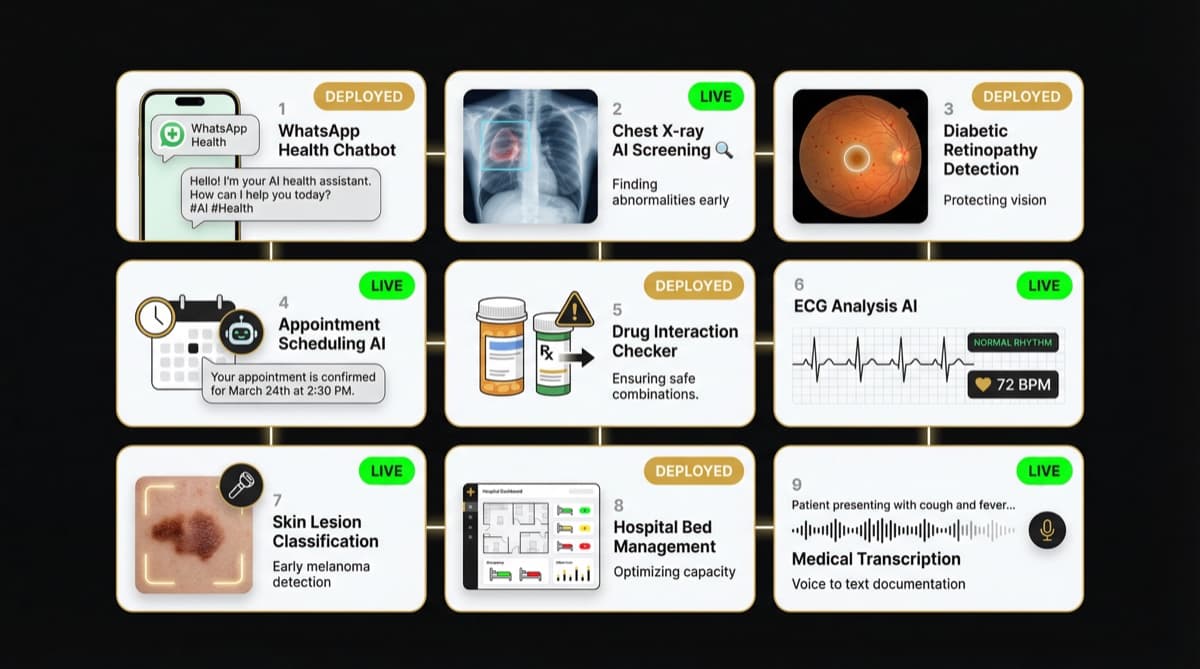
This isn't specific to radiology. The same pattern applies everywhere AI touches clinical work — diagnostics, triage, documentation, treatment planning.
Need help with this?
Our team specializes in healthcare branding. Get personalized advice in a free 15-minute call.
Book a free 15-minute callQ.Who Actually Benefits from AI in Healthcare?
Q.What Is Hospitals and PE Firms: The Primary Beneficiaries?
When a PE-backed hospital chain deploys AI across its radiology department:
Before AI: 10 radiologists x 100 studies/day = 1,000 studies. Radiology department cost: Rs 2.5 crore/year. Revenue from 1,000 studies/day.
After AI: 8 radiologists x 170 studies/day = 1,360 studies. Radiology department cost: Rs 2 crore/year (2 fewer FTEs) + Rs 15 lakhs AI tools. Revenue from 1,360 studies/day (+36%). Net value: +36% revenue, -18% cost = massive EBITDA gain. Value captured by: Hospital.
The PE firm that invested in hospital AI sees ROI through EBITDA expansion. The technology investment pays for itself within 12-18 months and generates returns thereafter.
Q.What Is Technology Companies: The Enablers?
AI healthcare companies (Qure.ai, SigTuple, 5C Network) capture subscription revenue from hospital deployments. Their business model depends on demonstrating productivity gains that hospitals can monetize — which means their incentive is aligned with hospital EBITDA, not doctor compensation.
Q.What Is Patients: Mixed Results?
Patients benefit from: faster report turnaround, fewer missed diagnoses (AI catches what tired eyes miss), and potentially wider access (AI enables screening in underserved areas).
Patients may not benefit from: the throughput pressure AI enables. When hospitals use AI-boosted efficiency to see more patients per doctor, consultation quality may suffer even as diagnostic accuracy improves.
Q.What Is Doctors: The Structural Losers?
Doctors don't lose their jobs. They lose their leverage. The scarcity premium that made specialized knowledge valuable gets diluted when AI can perform or assist with the routine components of that knowledge. And in a healthcare system where 50% of hospital costs are doctor compensation, any tool that reduces per-unit doctor cost is enormously attractive to employers.
Q.What Is Structural Mechanism: Scarcity to Abundance?
Medical specialties historically commanded premium compensation because expertise was scarce. A trained radiologist could read chest X-rays because they spent years learning to recognize patterns. That training created scarcity, and scarcity created value.
AI disrupts this by commoditizing the pattern recognition component — the routine part of the work. It doesn't commoditize the complex clinical judgment, the patient communication, or the ethical decision-making. But in volume-driven healthcare (which is most of Indian healthcare), routine pattern recognition represents 60-80% of the workload.
The result: The 60-80% of work that was routine becomes AI-assisted (fast, cheap, accurate). The 20-40% that requires genuine human expertise remains the doctor's domain. But compensation was based on 100% of the workload being human — and the renegotiation that follows favors the employer.
Q.How This Compares to PE-Driven Compensation Shifts?
The AI leverage shift and PE-driven compensation restructuring are structurally identical — they just use different mechanisms:
PE Compensation Shift: Revenue-share changes to fixed salary. Doctor's workload same or increased. Compensation decreased (capped variable pay). Hospital benefit: higher EBITDA margins. Doctor's leverage reduced (standardized contracts). Justification: "Market standardization."
AI Leverage Shift: Full reads change to AI-assisted validation. Doctor's workload same or increased. Compensation stagnant (no share of productivity gains). Hospital benefit: higher output per doctor, lower per-unit cost. Doctor's leverage reduced (scarcity premium erodes). Justification: "Technology is helping you."
Both mechanisms produce the same outcome: doctors generate more value for hospitals while capturing a smaller share of it.
Q.What Doctors Can Do About It?
- 1Build Unreplicable Skills
AI can read a chest X-ray. It can't build a patient relationship, navigate a complex clinical decision with incomplete information, or manage the emotional dimensions of a cancer diagnosis. Skills that AI can't replicate are your long-term moat.
- 1Own the Patient Relationship
If patients come to see you (not just your hospital), your value isn't reducible to AI-assisted productivity metrics. Building a personal brand, maintaining direct patient connections, and being the reason patients choose a facility — this is leverage that AI can't erode.
- 1Move Up the Complexity Chain
Routine diagnostic reads are most vulnerable to AI augmentation. Complex interventional radiology, multi-system diagnostic puzzles, rare presentations, and integrated clinical reasoning are least vulnerable. Position yourself at the complex end of your specialty.
- 1Understand the Economics
When your hospital deploys AI and expects you to "maintain" the new productivity baseline, you should understand what that baseline represents in revenue terms — and negotiate accordingly. If AI enables you to generate Rs 2 crore in annual revenue instead of Rs 1.3 crore, your compensation should reflect the value creation.
- 1Build Outside the System
Doctors who own clinics, build content platforms, develop health-tech products, or create educational businesses aren't subject to hospital EBITDA dynamics. Ownership is the structural solution to leverage erosion.
Frequently Asked Questions
Q: How does AI change doctor salaries?
A: Not through direct cuts — through the leverage shift. AI increases per-doctor productivity, and hospitals capture the productivity gains as EBITDA improvement rather than passing them to doctors as compensation increases. The effect is stagnant or slowly declining real compensation relative to the value doctors generate.
Q: Will AI create new medical jobs?
A: Yes — AI implementation requires clinical AI specialists, AI validation experts, and health informatics professionals. However, these new roles are fewer than the efficiency gains AI enables.
Q: Should I invest in learning AI?
A: Yes — but "learning AI" for a doctor means becoming AI-literate (understanding capabilities, limitations, and validation), not becoming a data scientist. The doctors who thrive in AI-augmented healthcare are those who can effectively work with AI tools while maintaining the clinical judgment that AI lacks.
Q: Is this inevitable or can it be changed?
A: The technology is inevitable. Who captures the value isn't. In systems where doctors have more bargaining power (unions, collective negotiation, ownership structures), productivity gains from AI can be shared. In India's PE-driven hospital system, the current structural trajectory favors hospitals over doctors.
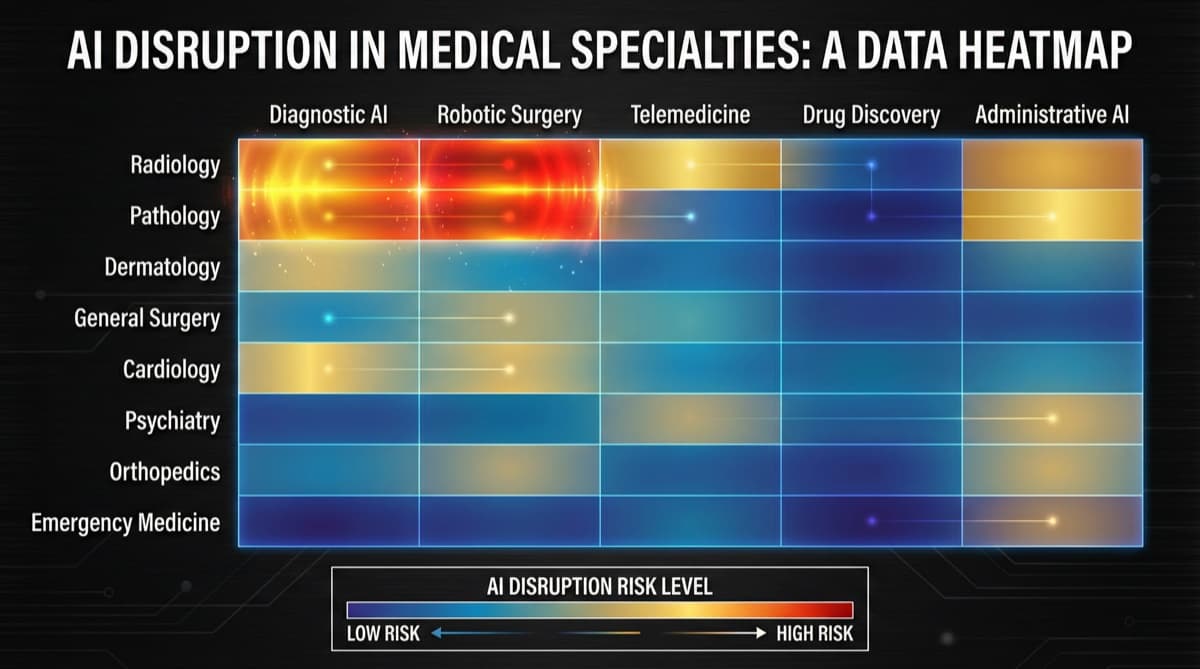
Q: What specialties are most AI-proof?
A: Specialties requiring complex clinical reasoning, physical procedures, patient relationships, and multi-system integration: surgical sub-specialties, complex internal medicine, critical care, psychiatry, and palliative care. The most AI-vulnerable: routine diagnostic interpretation, basic screening, and standardized protocol-driven care.
futurise. builds premium healthcare brands in 48 hours. Learn more at futurise.studio