Radiology, pathology, and diagnostic imaging will be the first medical specialties structurally disrupted by AI in India — not because AI replaces radiologists or pathologists, but because it shifts leverage from the doctor to the hospital. When AI software can flag abnormalities in X-rays, CTs, and MRIs with 95%+ accuracy, the radiologist doesn't become unnecessary — they become less scarce. And when scarcity decreases in a PE-backed hospital system optimized for EBITDA, the result isn't fewer radiologists — it's the same number of radiologists doing more work for the same or less pay. India's AI diagnostics market is projected to triple from $12.87 million (2024) to $44.87 million by 2030, and approximately 40% of Indian clinicians are now using AI technologies.
What Is the AI Impact Hierarchy — Which Specialties Get Hit First?
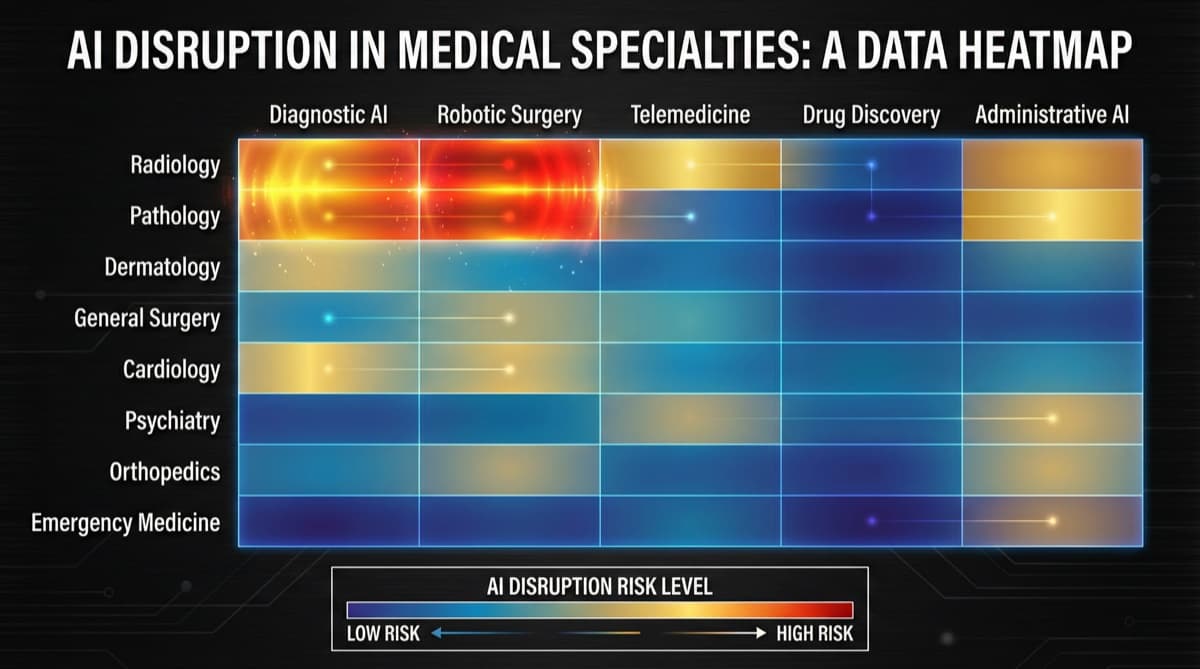
AI disruption follows a clear tier-based pattern. Tier 1: Immediate | Radiology, Pathology, Dermatology (diagnostics) | Pattern recognition from images — AI's core strength | Already happening (2024-2026) Tier 2: Near-term | Ophthalmology, Cardiology (diagnostics), Primary Care (triage) | Structured data + imaging + decision support | 2026-2028 Tier 3: Medium-term | Oncology, Psychiatry (screening), Emergency (triage) | Complex data integration + clinical decision support | 2028-2032 Tier 4: Long-term | Surgery, Critical Care, Complex Internal Medicine | Physical intervention + real-time judgment required | 2032+
How Is AI Already Disrupting Radiology and Pathology in India?
This disruption is not hypothetical — it's already underway. What AI Is Already Doing
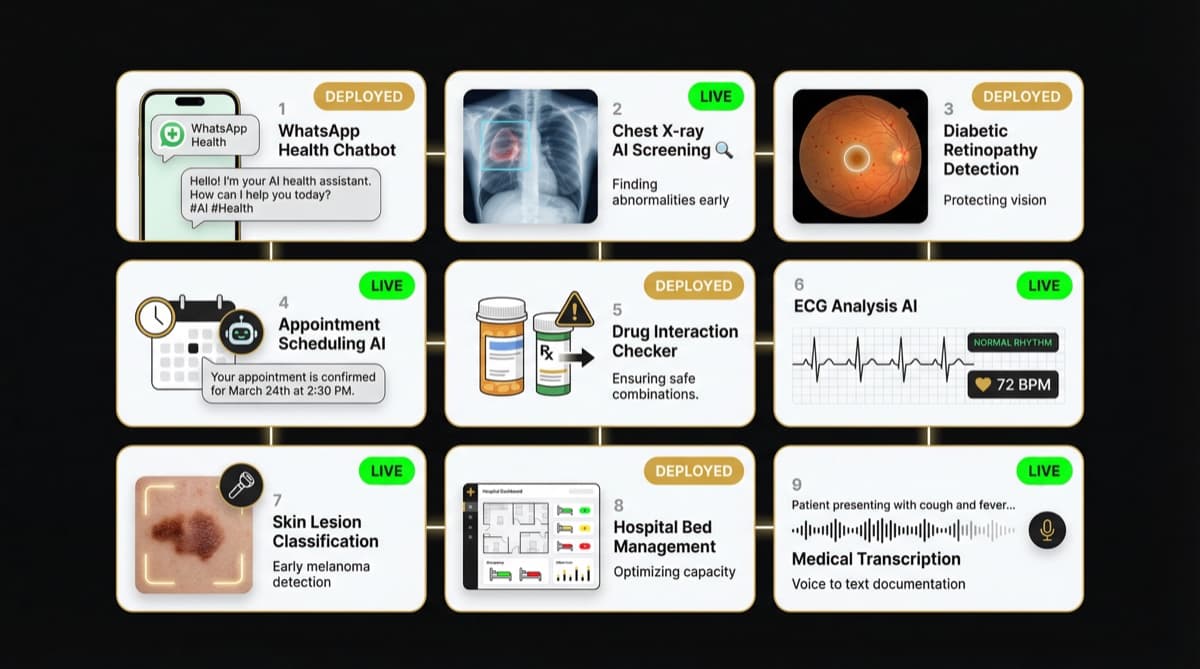
India's leading hospitals are deploying AI tools from companies like Qure.ai, Predible Health, and SigTuple:
- Chest X-ray screening: AI detects tuberculosis, pneumonia, and lung nodules with sensitivity comparable to radiologists
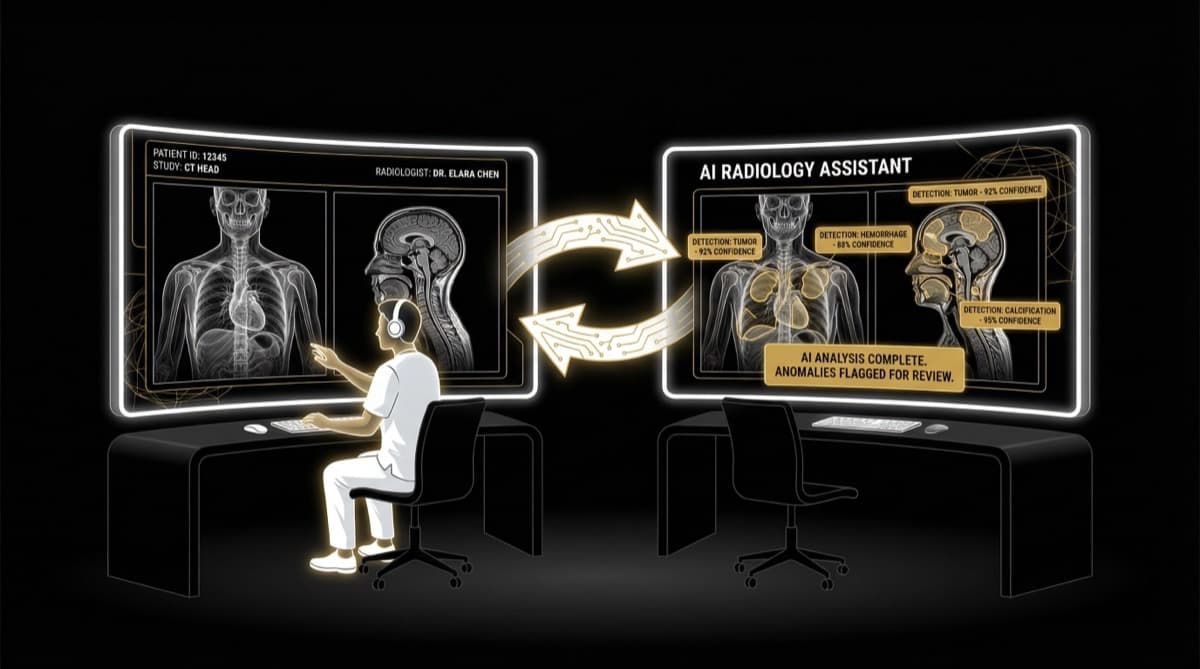
- CT scan analysis: AI algorithms identify stroke, hemorrhage, and pulmonary embolism and flag urgent cases for priority reading
- Mammography screening: AI-assisted breast cancer detection reduces missed diagnoses
- Pathology slides: Digital pathology with AI-assisted cell counting, tissue analysis, and cancer grading
The Structural Impact on Radiologists
Before AI: A radiologist reads 80-120 studies per day. Their scarcity (limited supply of trained radiologists) maintains their market value. Hospitals need them — and pay accordingly.
With AI: AI pre-screens studies, flags abnormals, and provides preliminary reads. The radiologist now reviews AI output rather than reading from scratch. Productivity increases to 150-200+ studies per day.
The leverage shift: The hospital captures the productivity gain. The radiologist processes 50-70% more studies but doesn't earn 50-70% more. Hospital revenue per radiologist increases. Radiologist compensation per study may decrease or stay flat while volume grows.
This is the three-phase pattern: Panic → Relief → Quiet Salary Cap.
- 1Panic: "AI will replace radiologists!"
- 2Relief: "AI is a tool that helps us, not replaces us."
- 3Quiet salary cap: AI-boosted productivity becomes the new baseline expectation. Hospitals expect more output per radiologist. New graduates enter a market where AI-assisted reading is standard — and negotiating power shifts to the employer.
How Does AI Change the Value Equation for Doctors?
The fundamental shift isn't about replacement — it's about who captures the value of increased productivity.
The Pre-AI Model
- Doctor's expertise is scarce → hospital needs the doctor → doctor has leverage → doctor captures a significant share of revenue
The Post-AI Model
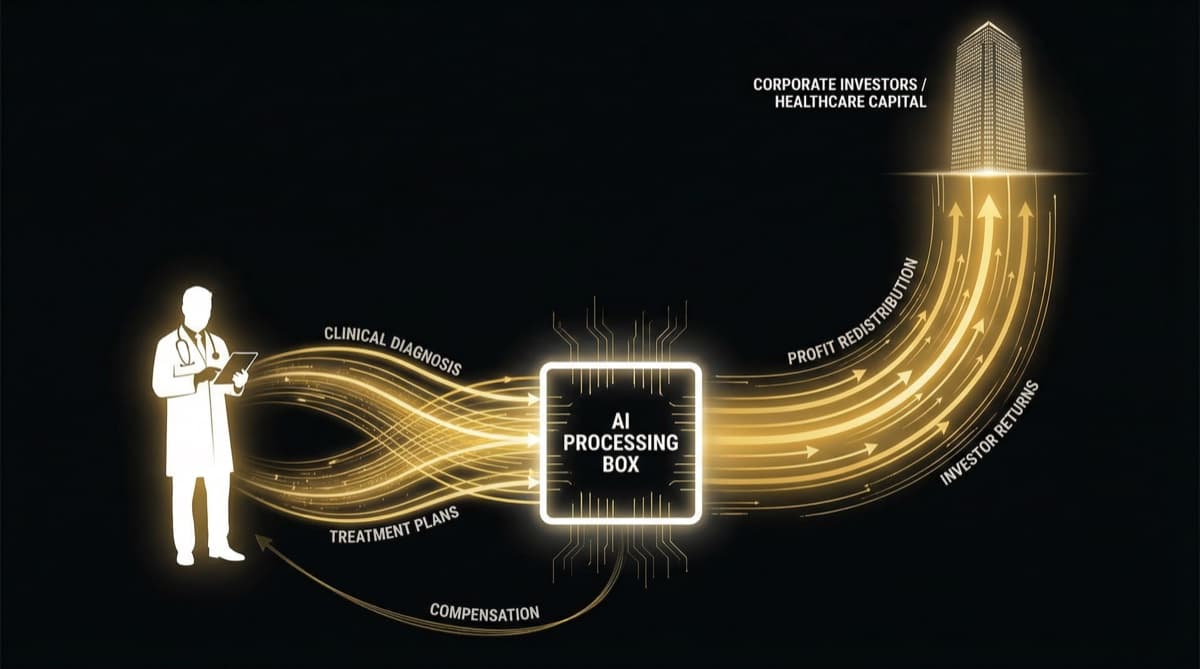
- AI reduces the scarcity premium → hospital captures efficiency gains → doctor becomes more productive but not proportionally richer → hospital margins improve
The Data At hospitals where AI-assisted radiology is deployed:
- Scan volume per radiologist increases 40-70%
- Turnaround time for reports decreases 50-60%
- Hospital diagnostic revenue grows 20-30%
- Radiologist compensation: flat or marginally increased
The productivity gains flow to the hospital's EBITDA, not to the doctor's paycheck. This is structurally identical to what PE-driven compensation restructuring does — but through technology rather than contract renegotiation.
What Does AI in Healthcare Mean for Different Career Stages?
The implications vary significantly by where you are in your career. Medical Students Choosing Specialties (2026)
Don't avoid radiology or pathology because of AI. These specialties aren't dying — they're evolving. The radiologist of 2030 needs to be an AI-literate imaging specialist, not just a film reader. Those who can work with AI, validate AI outputs, and handle cases AI can't manage will remain valuable.
Do consider: AI augmentation means the ceiling for how many studies one radiologist can manage increases. This could mean fewer total positions needed — or more volume handled per position at similar compensation.
Mid-Career Specialists (5-15 years experience)
If you're already in radiology or pathology, the immediate impact is: learn to work with AI tools or become less competitive. Hospitals that adopt AI will expect their radiologists to match the productivity benchmarks AI enables. Those who resist become cost-inefficient compared to AI-augmented peers.
Hospital Administrators / Practice Owners
AI is an infrastructure investment that increases revenue per doctor. The ROI on AI diagnostic tools comes from processing more studies without adding proportional radiologist headcount. For PE-backed hospitals, AI adoption is a margin expansion tool — not a quality improvement initiative (though quality may improve as a side effect).
Where Does AI in Healthcare Go Beyond Diagnostics?
Several clinical areas are next in line for AI integration. Primary Care Triage AI chatbots and symptom checkers are already routing patients before they see a doctor. In India, where the doctor-to-patient ratio forces 3-minute consultations, AI pre-triage could reduce the low-complexity patient load on doctors — freeing time for complex cases.
Ophthalmology Diabetic retinopathy screening through AI-analyzed retinal scans is among the most validated AI applications in medicine globally. In India, where diabetes affects 100+ million people and ophthalmologists are concentrated in cities, AI screening at PHC level could be transformative.
Cardiology AI-assisted ECG interpretation, echocardiogram analysis, and cardiac risk scoring are in active deployment. The structural impact mirrors radiology: more diagnostic volume per cardiologist, productivity gains captured by the hospital.
Mental Health AI-powered screening tools for depression, anxiety, and suicide risk are emerging. In a country where the psychiatrist-to-patient ratio is approximately 1:100,000, AI screening isn't threatening psychiatrists — it's creating demand for them by identifying patients who need care.
Frequently Asked Questions
Will AI replace doctors in India? No — AI will augment doctors, not replace them. But "augment" means something specific: AI increases the volume of work each doctor can handle, which shifts economic leverage from the doctor to the employer. You won't lose your job to AI. You might lose your salary premium to AI.
Is radiology a good career in India with AI? Yes — radiology is a growing field with increasing demand for diagnostic imaging. AI doesn't eliminate the need for radiologists; it changes what they do (from reading from scratch to validating AI-assisted reads). The key risk isn't unemployment — it's salary compression as AI reduces the scarcity premium that drove radiology compensation.
Which AI tools are Indian hospitals actually using in 2026? Qure.ai (chest X-rays, head CTs), Predible Health (cardiac CT), SigTuple (blood diagnostics), Niramai (breast cancer screening), Google Health (retinal screening), and various international tools from GE, Siemens, and Philips. Approximately 40% of Indian clinicians report using AI technologies in some capacity.
How should doctors prepare for AI in healthcare? Learn to work with AI tools — most leading radiology and pathology training programs now include AI literacy. Understand the limitations of AI (false positives, edge cases, bias in training data). Build skills that AI can't replicate: complex clinical reasoning, patient communication, ethical judgment, and multi-system integration.
Will AI affect doctor salaries in India? Not through direct salary cuts but through the leverage shift described above. When AI enables one doctor to do the work of 1.5, hospitals don't pay 1.5x — they may pay 1.0-1.1x while capturing the remainder as margin improvement. The salary impact is subtle, structural, and likely to compound over the next decade.
Need a website that converts patients? We build healthcare websites in 48-72 hours. Check our Web Launch package at futurise.studio/services