At least 118 medical students and doctors died by suicide in India between 2020 and 2022 — and that number is almost certainly an undercount due to systematic underreporting. Doctors in India face a suicide risk 2.5 times higher than the general population. An NMC survey in 2024 found that 1 in 3 postgraduate medical students had experienced suicidal ideation, over 10% had formulated a plan, and close to 5% had attempted suicide in the preceding year. These deaths are not random tragedies — they follow structural patterns: debt, overwork, medicolegal pressure, and a system that treats doctor mental health as irrelevant.
What Data Do We Have on Doctor Suicide in India — and Why Is It Incomplete?
The available data, while alarming, is almost certainly an undercount. Documented suicides (medical students + professionals, 2020-2022) | 118 fatal cases | LWW Archives of Medicine 2025 Suicide risk vs general population | 2.5x higher for doctors | PMC / Indian Journal of Psychiatry PG students with suicidal ideation | 1 in 3 (33%) | NMC Survey 2024 PG students who formulated a plan | Over 10% | NMC Survey 2024 PG students who attempted suicide | ~5% | NMC Survey 2024 Age profile | 50%+ under age 30 | LWW Archives 2025 Gender split (2016-2019 media reports) | 60% female, 40% male | PMC 2021 study From medical education institutions | 73% (22 of 30 in 2016-2019 study) | PMC 2021
Why the data is incomplete: India does not maintain a specific registry of doctor or medical student suicides. The 118 figure comes from media-reported cases — the actual number is almost certainly higher. Deaths classified as "accidental" or attributed to other causes, suicides in rural areas that don't make news, and families that choose not to report reduce the visible count.
What Are the Structural Causes of Doctor Suicide in India?
Doctor suicides in India follow identifiable structural patterns. Understanding these patterns is essential because the solution lies in changing the structures, not in asking individual doctors to be more resilient.
- 1The Debt-Income Trap
Private medical college fees range from Rs 10-25 lakhs per year for MBBS and significantly more for PG seats. A doctor graduating from a private medical college may carry Rs 50 lakhs-1 crore in educational debt. They then enter a job market where fresh MBBS salaries are Rs 40,000-90,000/month — often insufficient to service loan EMIs while covering living expenses.
The financial pressure is most acute in the first 5-8 years after graduation, which is precisely when clinical workload and career uncertainty are highest. The debt doesn't pause while you complete your residency at Rs 50-80K/month stipend.
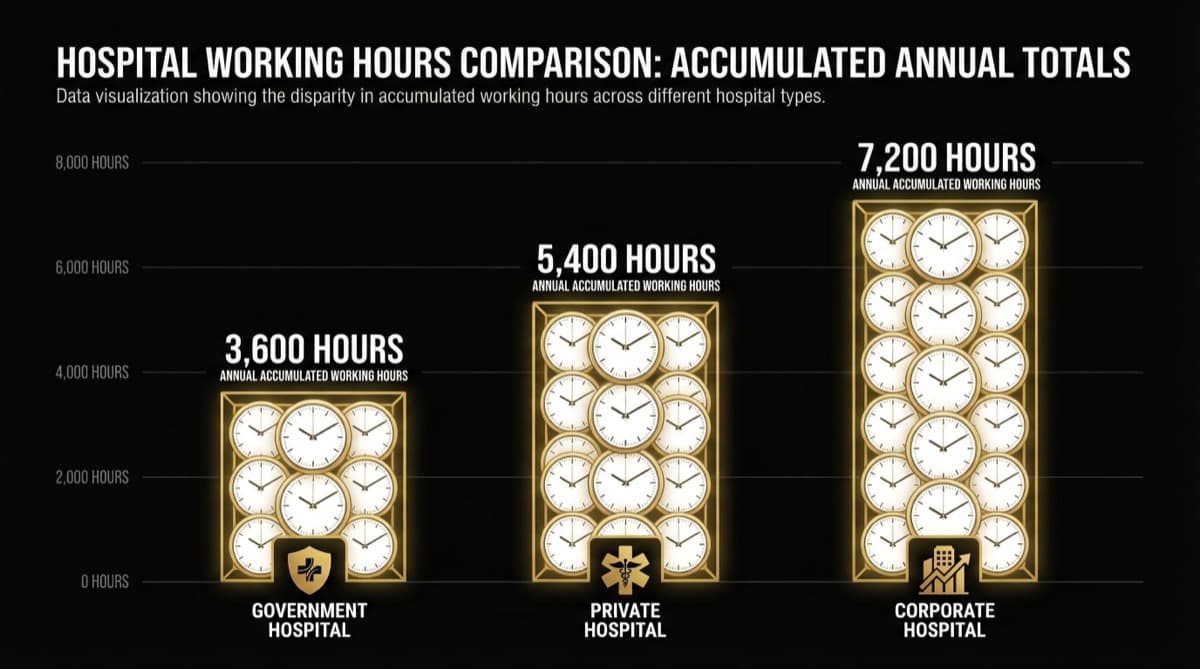
- 1The Working Hours Crisis
Resident doctors working 100-120 hours per week, with 36-hour continuous shifts, are in a state of chronic sleep deprivation. Sleep deprivation is a known risk factor for depression, anxiety, and suicidal ideation. When the NMC's own survey finds 1 in 3 PG students experiencing suicidal thoughts, the connection to 100-hour work weeks is structural, not coincidental.
- 1The Medicolegal Pressure
Doctors in India face increasing medicolegal threats — consumer protection cases, social media campaigns, WhatsApp group defamation, and the ever-present risk of workplace violence. 46.3% of doctors cite fear of violence as their primary stressor. For a profession already under extreme time and financial pressure, the addition of legal and physical threat creates a compounding stress architecture.
- 1The Academic Pressure Cooker
Medical education in India is intensely competitive at every stage — NEET UG, NEET PG, and within residency programs. The hierarchical culture of medical education often includes harassment, humiliation, and punitive supervision styles that would constitute workplace abuse in any other profession. Residents who report mistreatment risk academic retaliation from the supervisors who control their evaluations.
- 1The Absence of Support Systems
There is no mandatory mental health support infrastructure for doctors in India. No confidential counseling services in most medical colleges. No peer support programs. No structural acknowledgment that the profession itself creates mental health risk.
The stigma of seeking help is particularly acute in medicine — the very professionals trained to provide health care are culturally expected to be immune to needing it themselves.
What Is the Demographic Profile of Doctors at Risk?
The available data reveals concerning patterns:
Young doctors are most vulnerable. More than 50% of documented suicides occurred in individuals under 30 — the training and early career phase where debt, workload, and career uncertainty converge with minimal financial reserves and professional autonomy.
Women are disproportionately represented. In the 2016-2019 documented cases, 60% were female. Female doctors face additional structural pressures: gender-based harassment in medical institutions, safety concerns (72% of female doctors in Tier 2/3 cities report feeling unsafe), and career penalties for marriage and motherhood.
Medical education institutions are the primary setting. 73% of documented cases (in the 2016-2019 data) came from medical education institutions — medical colleges and teaching hospitals where the combination of academic pressure, working hour violations, and power hierarchies is most intense.
What Structural Interventions Are Needed to Address Doctor Suicide?
This section deliberately focuses on systemic solutions, not individual coping strategies. When a structural problem produces predictable outcomes, the solution must be structural.
Working hours enforcement with teeth. Tie medical college accreditation to independently verified compliance with NMC's 48-hour weekly limit and 12-hour shift cap. Financial penalties for violations. Annual compliance audits.
Mandatory mental health services. Every medical college and teaching hospital should be required to provide confidential, free, 24/7 mental health support for residents and students — provided by professionals outside the institution's reporting hierarchy.
Anti-harassment mechanisms. Independent complaint systems for residents facing academic harassment, with protection against retaliation. The current system where the harasser also controls academic assessment makes reporting structurally impossible.
Financial reform. Capping capitation fees, expanding government medical seats, and creating loan restructuring programs tied to public service can address the debt-income trap that creates financial desperation.
Data collection. Establish a national registry of medical professional suicides with standardized reporting requirements. You cannot address a problem you don't measure.
Frequently Asked Questions
What is the suicide rate among doctors in India compared to the general population? Doctors in India face a suicide risk approximately 2.5 times higher than the general population. India's general suicide rate was 12.4 per 100,000 in 2022 (the highest recorded year). The exact doctor-specific rate is difficult to calculate due to underreporting, but available data consistently shows elevated risk.
Are medical student suicides increasing in India? The available data suggests yes, though measurement challenges make definitive trend analysis difficult. NMC's 2024 finding that 1 in 3 PG students have experienced suicidal ideation is alarming. June 2025 alone saw multiple reports of resident doctors taking their lives.
Why are female doctors at higher risk? Structural factors include: gender-based harassment in medical institutions, safety concerns in hospitals and hostels, additional cultural pressures around marriage and family expectations, and the "motherhood penalty" that threatens career continuity. Female doctors in Tier 2/3 cities report feeling unsafe at rates 10% higher than metro counterparts.
What should I do if a colleague seems to be struggling? Ask directly and listen without judgment. Don't try to be their therapist — connect them with professional support. Vandrevala Foundation Helpline (1860-2662-345, 24/7) and iCall (9152987821) provide confidential support. Your role is to bridge the gap between their struggle and professional help.
Is NMC doing anything about this? NMC has acknowledged the problem — their own 2024 survey produced the suicidal ideation data. They've issued PGMER Guidelines limiting duty hours. But enforcement remains the gap. Guidelines without penalties, monitoring, and accountability mechanisms are aspirational documents, not structural solutions.
futurise. builds premium healthcare brands in 48 hours. Learn more at futurise.studio