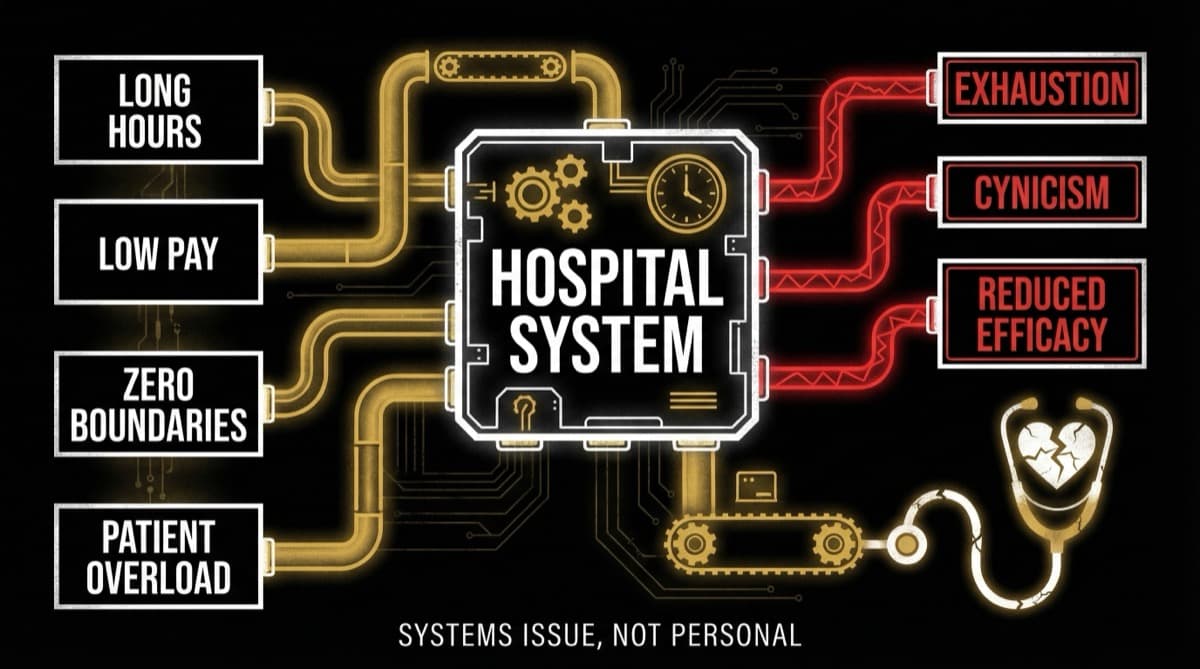
Indian hospitals exploit resident doctors through 36-hour shifts, 100-120 hour work weeks, and unpaid overtime — then label it "training" and "clinical exposure." According to NMC survey data from 2024, 1 in 3 postgraduate students have experienced suicidal ideation, and first-year residents make 36% more serious medical errors during extended shifts. The NMC's own PGMER Guidelines (2023) cap shifts at 12 hours and weekly hours at 48 — regulations that RTI data confirms are systematically violated at premier institutions including AIIMS and AFMC. This isn't a training model — it's a staffing model that uses the word "training" to justify unpaid labor.
What Is the Gap Between Working Hour Guidelines and Reality?
The contrast is stark. Maximum 48 hours/week (NMC PGMER 2023) | Average 100-120 hours/week in government hospitals Maximum 12 hours per continuous shift | 36-hour continuous shifts routinely documented Mandatory rest between shifts | Post-call duties immediately after night shifts Duty hour compliance for accreditation | No effective monitoring or enforcement mechanism Training-focused residency | Service-heavy workload with minimal structured teaching
RTI responses from AIIMS Bhubaneswar and AFMC Pune confirm that junior doctors are working up to 36-hour shifts without adequate rest — directly contravening the regulations that NMC itself issued.
How Does "Training" Become a Staffing Strategy?
The structural mechanism is straightforward: Indian teaching hospitals are chronically understaffed, and resident doctors fill the gap as cheap labor labeled "trainees."
The staffing math: A government teaching hospital needs a certain number of doctors to cover wards, emergency departments, OPDs, and surgical lists 24/7. Hiring enough qualified staff at consultant-level salaries would be expensive. Instead, the system fills these positions with PG residents who receive stipends of Rs 50,000-80,000/month — a fraction of what consultants would cost.
The "training" justification: Every hour a resident spends managing ward patients, completing discharge summaries, running between departments, and handling routine procedures is categorized as "clinical training." The distinction between genuine learning (supervised procedures, case discussions, research) and service work (administrative tasks, routine ward management, repetitive procedures) is never formally tracked.
The bondage system: After completing residency, many graduates are bound by service bonds of 1-3 years, requiring them to work at the same institution or government facilities at below-market compensation. This extends the exploitation window beyond the residency itself.
What Is the Real Cost of 36-Hour Shifts?
The costs fall on residents, patients, and the system. Cost to Residents
- 42% meet clinical burnout criteria within their residency period (IMA-Goa/Sangath 2024)
- 1 in 3 PG students have experienced suicidal ideation (NMC survey 2024)
- Over 10% had formulated a suicide plan, and close to 5% had attempted suicide in the preceding year
- 86% of young doctors believe excessive duty hours directly harm their mental health (Knya Vitals 2025)
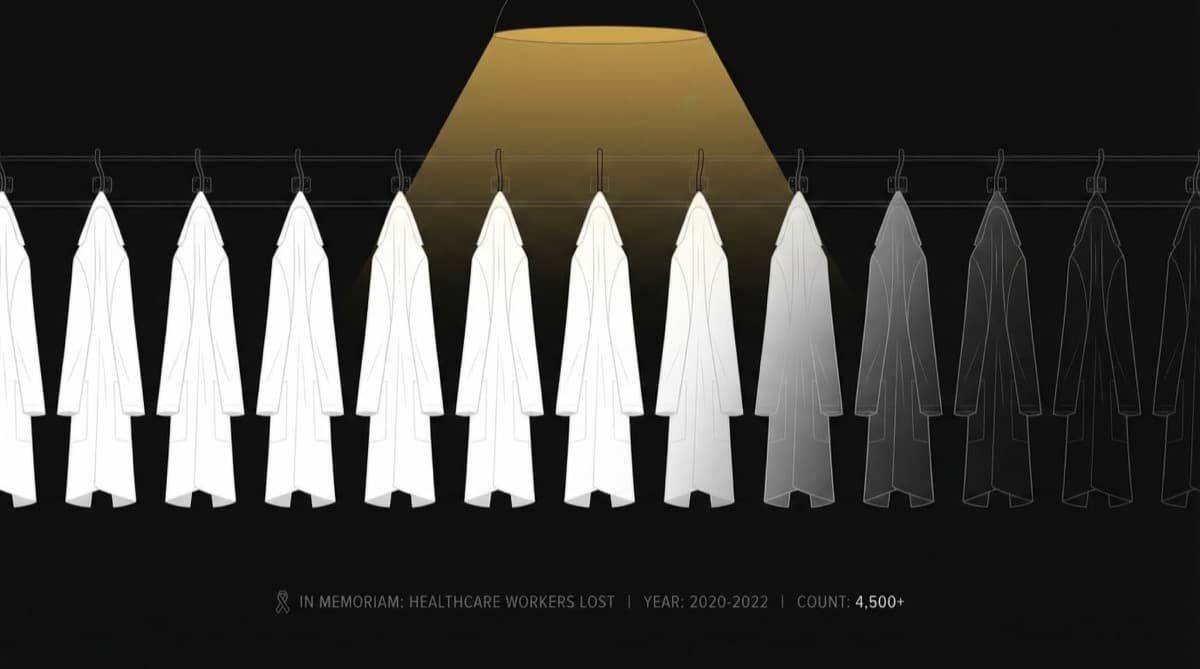
- 118 fatal suicides among medical students and professionals were documented over 3 years (2020-2022), with more than 50% occurring before age 30
Cost to Patients
- 36% more serious medical errors during extended shifts (compared to shorter shifts)
- Sleep-deprived doctors make worse clinical decisions — this is not debatable, it's established science
- High resident turnover in exhausted departments means patients see different doctors at each visit, losing continuity
- The doctor who performs your surgery at hour 30 of a shift is not the same doctor who started at hour 1
Cost to the System
- Burnout during residency drives doctors away from public service — the very system that trained them
- 70% of young doctors (25-34) regret personal sacrifices made for medicine
- The doctors most likely to leave India are those who experienced the worst working conditions during training
- Institutions that overwork residents are creating the brain drain they then complain about
Why Don't Residents Speak Up About Working Conditions?
Multiple structural forces prevent it. Academic power dynamics: Your academic supervisor controls your training assessment, exam recommendations, and career trajectory. Complaining about working conditions to the person who grades your performance creates an obvious conflict.
Cultural framing: Medical culture frames endurance as virtue. "I survived 36-hour shifts, so should you" is not just a belief — it's an identity. Residents who push back are labeled as lacking dedication, not as advocating for evidence-based work practices.
ESMA restrictions: The Essential Services Maintenance Act restricts healthcare worker strikes in many states. Resident doctor associations can negotiate, but their leverage is limited by legal constraints on collective action.
Bond obligations: Residents under service bonds face financial penalties for leaving — creating a structural lock-in that reduces their bargaining power.
Replacement fear: In a system with more medical graduates than training positions, the implicit threat is always present: if you won't do it, someone else will.
What Would a Real Training Model Look Like?
Countries that have reformed resident working conditions show it's possible without compromising training quality:
EU Working Time Directive: Caps doctor hours at 48/week with mandatory rest periods. European surgical training outcomes are comparable to or better than systems with unlimited hours.
US ACGME Regulations (post-2011): Caps first-year residents at 16-hour shifts and all residents at 80 hours/week. Studies show no deterioration in clinical competency.
What India would need:
- Independent working hours monitoring (not self-reported by the institution)
- Accreditation tied to verified duty hour compliance
- Financial penalties for institutions that systematically violate guidelines
- Separation of "training hours" (supervised learning) from "service hours" (staffing functions)
- Whistleblower protections for residents who report violations
Frequently Asked Questions
Is working 36-hour shifts actually illegal in India? It violates NMC's PGMER Guidelines (2023), which cap continuous shifts at 12 hours and weekly hours at 48. However, these guidelines lack effective enforcement mechanisms. A Supreme Court petition (United Doctors Front vs Union of India) seeks to make these limits legally binding with penalties for violation.
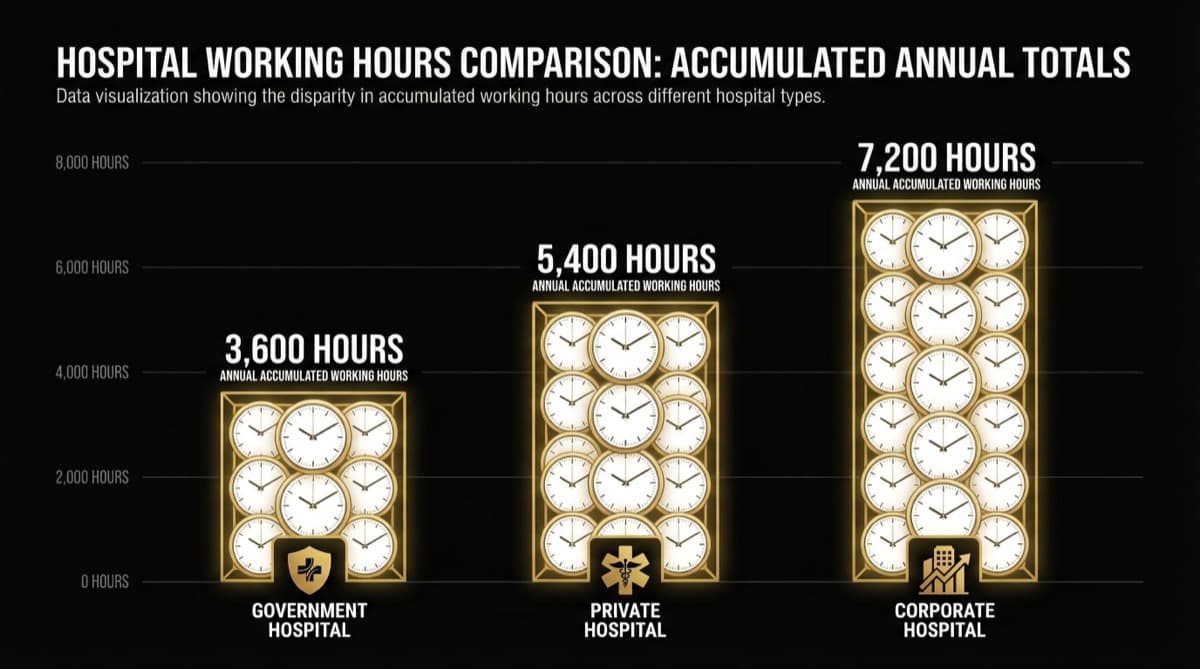
Do private hospital residents face the same working hour violations? Private medical colleges and corporate hospitals vary widely. Some maintain better hour compliance than government institutions; others are worse. The common denominator is that residents everywhere are treated primarily as a staffing resource rather than as learners.
Are residents paid for overtime in India? No. Resident stipends are fixed regardless of hours worked. A resident working 120 hours/week receives the same stipend as one working 48 hours. There is no overtime pay framework for medical residents in India.
Does the NMC actually act on working hour complaints? Sporadically. NMC has acknowledged violations at specific institutions (AIIMS Bhubaneswar, AFMC Pune) after RTI revelations, but systemic enforcement remains absent. No medical college has lost accreditation specifically for duty hour violations.
What can resident doctors do right now? Document your hours systematically (dates, shift start/end, breaks). Share documentation with resident doctor associations. Support the Supreme Court petition for enforceable working hour limits. And most importantly — recognize that your exhaustion is a system failure, not a personal one.
futurise. builds premium healthcare brands in 48 hours. Learn more at futurise.studio