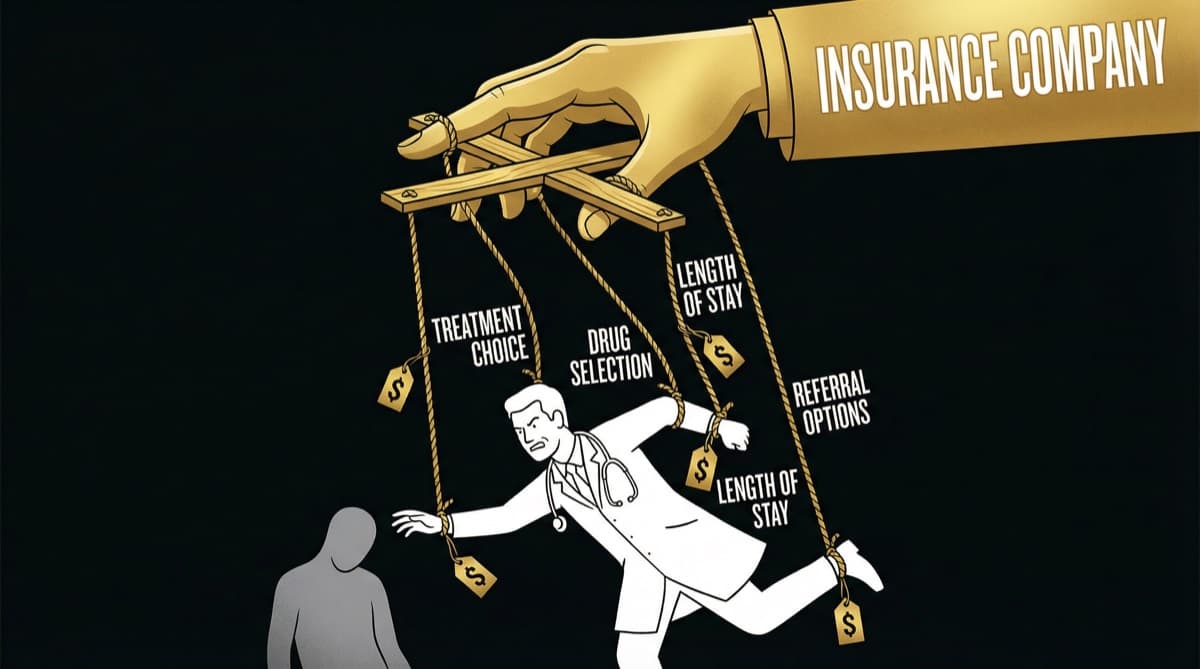
Insurance companies rejected health claims worth Rs 30,000 crore in FY 2024-25 — a 15% increase from the previous year. For doctors, every rejected claim means lost revenue, strained patient relationships, and hours of administrative work. The structural solution isn't working harder on paperwork — it's understanding why rejections happen and building a documentation system that prevents them. Here's the framework that reduces claim rejections from a daily frustration to a rare exception.
Why Do Insurance Claims Get Rejected — What Are the Structural Reasons?
Claim rejections aren't random — they follow predictable patterns driven by how insurance companies evaluate claims.
Pre-existing condition not disclosed | Most common | Low (patient disclosure issue) | Document thorough medical history at admission Treatment not medically necessary | Very common | High | Clinical justification in notes + investigation reports Procedure not covered under policy | Common | Medium | Verify policy coverage before procedure Insufficient documentation | Common | High | Follow the documentation framework below Waiting period violation | Common | Low | Check policy start date and waiting periods Room rent sub-limit exceeded | Common | Low (billing issue) | Counsel patient on room category at admission Non-compliance with pre-authorization | Common | High | Never skip pre-authorization for planned admissions Coding errors (wrong ICD/CPT codes) | Moderate | High | Verify procedure codes match clinical documentation Policy lapsed or expired | Moderate | Low | Verify active policy before admission
Key insight: Of the top 9 rejection reasons, 4 are within the doctor's direct control through better documentation and process compliance. Another 3 can be mitigated with admission-time verification. Only 2 (pre-existing condition non-disclosure and policy lapse) are genuinely outside the doctor's control.
What Documentation Framework Prevents Insurance Claim Rejections?
The most effective framework is the CLAIM Method. The CLAIM Method
C — Clinical History (Detailed) Document the complete presenting complaint, duration, progression, and previous treatments. For conditions that may be challenged as pre-existing, explicitly note: "Patient reports no prior history of [condition]" or "Patient reports [condition] diagnosed [date] at [facility]."
L — Logical Connection (Diagnosis to Treatment) Every investigation and treatment must logically connect to the documented diagnosis. If you order an MRI for a knee pain patient, your notes should show: symptoms → examination findings → clinical diagnosis → investigation ordered → findings → treatment plan. Insurance reviewers look for gaps in this chain.
A — Authority (Investigations and Evidence) Attach all investigation reports that support medical necessity. A claim for appendectomy supported by ultrasound showing inflamed appendix + elevated WBC + clinical tenderness gets approved. A claim with just "clinical diagnosis of appendicitis" gets questioned.
I — Informed Consent (Documented) Complete informed consent documenting: diagnosis explained, treatment options discussed, chosen treatment and rationale, risks explained, patient agreement. This protects against both medicolegal risk and insurance queries about treatment appropriateness.
M — Medical Necessity Statement For any procedure that might be questioned, include an explicit statement: "This procedure is medically necessary because [specific clinical reason]. Conservative management was [tried and failed / not appropriate because...]." This preempts the most common subjective rejection reason.
How Does Pre-Authorization Prevent Claim Rejection?
For planned (elective) admissions, pre-authorization is your primary defense against claim rejection.
What to Include in Every Pre-Authorization Request
- 1Patient demographics and policy details (verified, not assumed)
- 2Clinical diagnosis with ICD-10 code
- 3Planned procedure with CPT/hospital code
- 4Medical necessity justification (2-3 sentences connecting diagnosis to procedure)
- 5Investigation reports supporting the diagnosis
- 6Estimated cost breakdown within package rate
- 7Expected length of stay
Pre-Authorization Best Practices
- Submit 48-72 hours before planned admission — not the day before
- Follow up on pending approvals — don't assume silence means approval
- Get approval in writing (email/portal confirmation) — verbal approvals are not evidence
- If downgraded (insurer approves a lower procedure than recommended), document your disagreement and clinical rationale before proceeding
- For emergency admissions, submit retrospective authorization within 24 hours with full clinical justification for emergency status
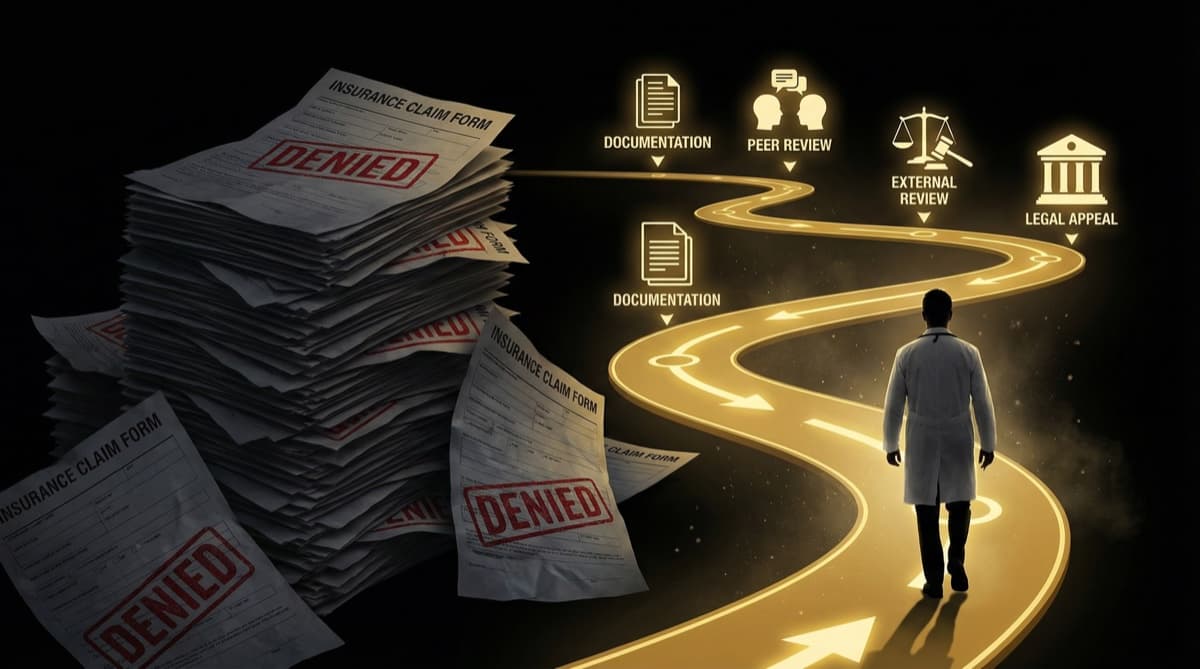
What Should You Do When a Claim Gets Rejected?
Follow a structured appeal process. Step 1: Understand the Rejection
Read the rejection letter carefully. Identify the specific reason code. Common codes:
- "Medically not necessary" — needs clinical justification
- "Pre-existing condition" — needs evidence of first diagnosis timing
- "Documentation insufficient" — needs specific missing documents
- "Not covered under policy" — needs policy review and possible patient escalation
Step 2: Prepare the Appeal
For each rejection reason, prepare a targeted response:
For "medically not necessary" rejections:
- Attach all investigation reports supporting the diagnosis
- Include clinical photographs if relevant (wound status, imaging findings)
- Reference clinical guidelines (e.g., "As per [specialty society] guidelines, [procedure] is indicated when [criteria], all of which are met in this case")
- Add a medical necessity statement from the treating consultant
For "insufficient documentation" rejections:
- Provide the specific documents requested
- Add a summary letter connecting all documents to the clinical narrative
- Since IRDAI's 2024 regulation, insurers can no longer reject claims solely for documentation gaps — cite this regulation in your appeal
For "pre-existing condition" rejections:
- Provide evidence of first diagnosis date and treatment history
- If the condition was genuinely new, provide a statement from the treating doctor with supporting investigations showing no prior evidence
- If the condition was pre-existing but policy has crossed the waiting period, demonstrate policy tenure
Step 3: Escalation Pathway
- 1TPA/Insurer grievance cell — first appeal (response within 15 working days)
- 2Insurance company grievance officer — if TPA response is unsatisfactory
- 3IRDAI Integrated Grievance Management System (IGMS) — regulatory complaint (portal: igms.irda.gov.in)
- 4Insurance Ombudsman — for claims up to Rs 30 lakhs (free, no lawyer needed)
- 5Consumer Court — for claims exceeding Rs 30 lakhs or after ombudsman failure
How Can You Build a Rejection-Proof Medical Practice?
It requires systems at two levels. At the Hospital Level
- Designate a trained insurance coordinator for every ward
- Create template documentation checklists for the 20 most common procedures
- Review rejection patterns monthly — most hospitals find 60-70% of rejections come from 3-4 recurring reasons
- Train admission staff to verify policy details, coverage limits, and room category sub-limits before admission
At the Doctor Level
- Spend 3 extra minutes per admission on documentation — it saves hours of appeal work later
- Always document the medical necessity statement for any procedure that could be questioned
- Use ICD-10 codes correctly — coding errors are an easily preventable rejection cause
- For high-value procedures, call the TPA medical officer to discuss the case before submission
Frequently Asked Questions
What percentage of health insurance claims get rejected in India? Approximately 15-20% of health insurance claims face some form of rejection or reduction. In FY 2024-25, rejections totaled Rs 30,000 crore. IRDAI data shows rejection rates have been increasing year-over-year, driven partly by stricter insurer scrutiny and partly by documentation gaps.
Can IRDAI's new regulation prevent documentation-based rejections? IRDAI's 2024 regulation states that no claim shall be rejected solely for "want of documents." However, insurers can still request additional documents and reject claims for other reasons (medical necessity, pre-existing conditions, policy exclusions). The regulation reduces one category of rejection but doesn't eliminate the structural causes.
How long does the insurance appeal process take? TPA/insurer response: 15-30 working days. IRDAI complaint: 30-90 days. Insurance Ombudsman: 2-3 months. Consumer Court: 6-18 months. The process is slow, which is why prevention (proper documentation) is far more effective than cure (appeals).
Should I stop seeing insured patients to avoid rejections? No — insurance patients represent a growing share of hospital revenue (30-40% in corporate hospitals). The solution is building documentation systems that minimize rejections, not avoiding insured patients. Hospitals with strong insurance processes achieve rejection rates below 5%.
What documentation standard should I follow? Follow the CLAIM method: Clinical history, Logical connection (diagnosis to treatment), Authority (investigation evidence), Informed consent, Medical necessity statement. This covers the most common rejection triggers and takes only 3-5 extra minutes per case.
futurise. builds premium healthcare brands in 48 hours. Learn more at futurise.studio