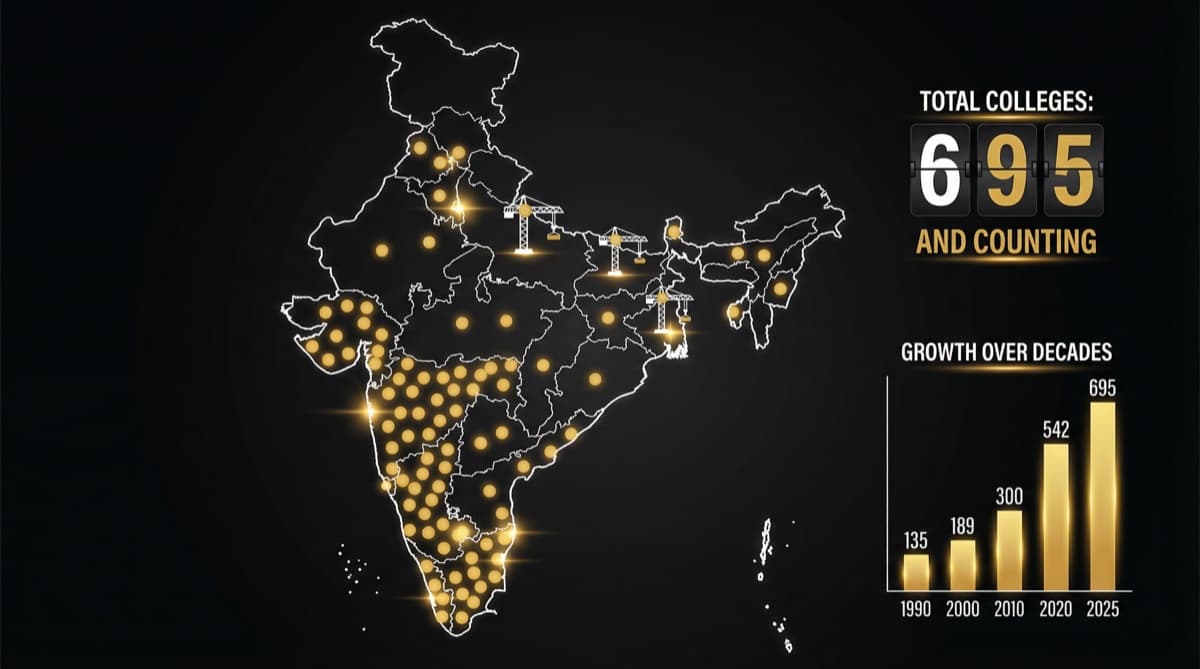
India has over 780 medical colleges with approximately 1,18,000 MBBS seats as of 2026 — up from 381 colleges with 49,000 seats in 2014. That's a doubling in just 12 years. But this growth isn't driven by healthcare need — it's driven by state politics (new colleges win votes), private investment (medical education is a Rs 50,000 crore+ industry), and a regulatory environment that approves colleges faster than it can ensure quality. The result: more graduates, but the same doctor distribution problems, the same specialist shortages in rural India, and starting salaries that haven't moved in a decade.
What Does the Growth Trajectory of Indian Medical Colleges Look Like?
The acceleration over the past two decades is dramatic. 2004 | ~240 | ~28,000 | ~25,000 | Organic growth 2010 | ~335 | ~42,000 | ~38,000 | Private college expansion begins 2014 | ~381 | ~49,000 | ~45,000 | NMC precursor policies 2018 | ~529 | ~72,000 | ~65,000 | State-driven expansion 2022 | ~660 | ~97,000 | ~90,000 | Post-COVID acceleration 2026 | ~780+ | ~1,18,000 | ~1,10,000 | Continued expansion
The acceleration is unmistakable: India added 400+ medical colleges in 12 years — more than the total that existed in 2004. MBBS seat capacity grew 140% while the population grew approximately 15% in the same period.
Why Does the Number of Medical Colleges Keep Growing?
Four structural forces drive continuous expansion. 1. Political Economics
Medical colleges are politically valuable assets. A new medical college in a constituency signals "development" and healthcare commitment. State governments approve colleges because:
- New colleges create jobs (faculty, staff, construction)
- They bring a teaching hospital to underserved areas (political goodwill)
- They signal healthcare investment to voters
- MPs and MLAs can claim credit for healthcare expansion
The political incentive is to announce and approve colleges — not to verify their quality or assess whether the market needs more graduates.
- 1Private Investment Returns
Medical education is among the most profitable education sectors in India. A 150-seat private medical college at average fees of Rs 15 lakhs/year generates Rs 22.5 crore annually in fee revenue from MBBS alone. Add PG seats, hospital revenue, and other programs, and the annual revenue of a well-run private medical college can exceed Rs 50-100 crore.
The capital investment is significant (Rs 100-300 crore for land, building, hospital, and equipment), but the return timeline is 7-10 years — attractive for investors.
- 1Regulatory Tailwinds
NMC replaced MCI in 2019, and the new framework was designed to be more permissive in college approvals. The stated goal was to increase doctor supply. The outcome: faster approvals, more private colleges, and less stringent quality gatekeeping during the expansion phase.
- 1The Narrative of Doctor Shortage
India's doctor-to-population ratio of 1:834 (often cited as below WHO's 1:1,000 recommendation) creates a persistent narrative that the country needs more doctors. This narrative justifies continuous seat expansion — even though the actual problem is distribution (70% of doctors in cities, 70% of population outside them), not absolute numbers.
Where Are the New Medical Colleges Located — and Where Are They Not?
The expansion isn't uniform. New colleges cluster in states where political and economic conditions favor them:
States with highest expansion: Uttar Pradesh, Madhya Pradesh, Rajasthan, Karnataka, Tamil Nadu, and Maharashtra have added the most colleges. These states combine large populations (political incentive), available land (practical requirement), and investor interest (economic incentive).
States underserved despite expansion: Northeastern states, smaller Union Territories, and states with less investor-friendly environments have fewer new colleges. The areas that most need doctors often get fewer medical colleges — because the economics of medical education favor populous, urbanized states.
Urban-rural mismatch: Most new private colleges are located in or near cities — because that's where patients (for the teaching hospital), faculty (who prefer urban living), and students (who prefer urban training) can be found. The rural doctor shortage persists because colleges aren't built where rural doctors are needed.
What Has Medical College Growth Achieved — and What Hasn't It?
What It Has Achieved
- More MBBS graduates: From ~25,000/year (2004) to ~1,10,000/year (2026) — a 4x increase
- More PG seats: PG capacity expanded alongside MBBS, though at a slower rate (~65,000 PG seats vs 1,18,000 MBBS seats)
- More healthcare infrastructure: Teaching hospitals attached to new colleges add clinical capacity in areas that previously had none
- More competition: Theoretically, more doctors should improve access and quality through market competition
What It Hasn't Achieved
- Rural specialist shortage unchanged: 88% specialist vacancies in rural community health centres persist despite doubling graduate output. Production ≠ distribution
- Starting salaries frozen: More graduates = more supply = more employer power = stagnant starting salaries at Rs 40-60K/month for a decade
- Quality variation: The fastest-growing segment (private colleges) has the widest quality variation. Some are excellent; others lack adequate clinical training volume
- NEET PG seat vacancies: 18,000+ vacant PG seats suggest that seat creation has outpaced the number of candidates willing to pay private PG fees
- Doctor-to-population ratio still below target in rural areas: The national average masks distribution failures
Does More Medical Colleges Mean Better Quality?
More colleges doesn't necessarily mean more good doctors. Quality of medical education depends on:
Clinical volume in the teaching hospital. A college whose hospital sees 500 patients/day provides vastly different training than one seeing 50. Many newer private colleges struggle with patient volume because the teaching hospital hasn't established community trust.
Faculty quality and availability. NMC requires minimum faculty numbers, but enforcement is inconsistent. "Ghost faculty" — professors who exist on paper but don't teach — is a documented problem. The rapid expansion created demand for medical teachers that outstripped supply.
Infrastructure and equipment. Labs, libraries, simulation centres, and diagnostic equipment require ongoing investment. Some private colleges invest adequately; others cut corners after receiving approval.
Frequently Asked Questions
How many medical colleges are in India in 2026? Approximately 780+ medical colleges with approximately 1,18,000 MBBS seats. This includes roughly 310 government colleges and 470+ private colleges (including deemed universities).
Is India producing enough doctors? India is producing enough graduates in absolute numbers — the issue is distribution. 70% of doctors practice in urban areas that serve 30% of the population. Rural areas face severe shortages despite total graduate numbers being adequate. The problem is where doctors choose to work, not how many are trained.
Are private medical colleges good? Quality varies enormously. Top private colleges (Kasturba Medical College, St. John's, Christian Medical College) are among India's best. Newer private colleges approved in the expansion wave range from excellent to inadequate. The key differentiators are clinical volume, faculty quality, and institutional commitment to training.
Will more medical colleges solve the doctor shortage? No — not by themselves. The shortage is primarily a distribution and retention problem. Adding more colleges in urban areas produces more urban doctors. Solving rural shortages requires incentive restructuring (higher rural salaries, better infrastructure, career growth pathways) — not just more graduates.
Should the government stop approving new medical colleges? Not necessarily — but the focus should shift from quantity to quality and distribution. New colleges in genuinely underserved areas with adequate clinical volume and faculty are valuable. New colleges in already-saturated urban markets that primarily serve as investment vehicles contribute to oversupply without addressing access gaps.
futurise. builds premium healthcare brands in 48 hours. Learn more at futurise.studio