On this page
The Specialty Nobody Wants (But Everyone Needs)
Emergency Medicine has the highest demand-supply gap in Indian medicine: 72% unfilled positions in hospitals, +8.2% annual demand growth, and acute staffing crises in 80% of government EDs. Yet it's chosen by <3% of graduating medical students. Why? Because it combines the highest workload, lowest compensation compared to effort, and highest violence risk of any specialty. It's a market failure where supply can't meet demand, and doctors who choose it do so by default (guaranteed job) rather than by preference.
Q.What Is Structural Mechanism 1: Demand-Supply Crisis by Metrics?
| Metric | Emergency Medicine | Surgery | Cardiology | Dermatology | What It Means |
|---|---|---|---|---|---|
| Government Hospital Vacancy Rate | 72% (unfilled ED positions) | 42% | 28% | 12% | EM has 3x more unfilled positions than Dermatology |
| Private Hospital Vacancy Rate | 65% | 35% | 20% | 8% | EM shortage across all hospital types |
| Annual Demand Growth | +8.2% | +3.1% | +4.5% | -0.8% | EM demand growing; others stagnant/declining |
| Job Applicants Per Position | 0.4 (0.4 doctors per job) | 2.1 | 1.8 | 8.5 | EM positions outnumber applicants; others have surplus applicants |
| Time to Fill Position | 1-2 weeks (perpetual recruitment) | 2-3 months | 2-4 months | 6-12 months | EM hospitals hire whoever applies; others selective |
| Average Retention in Role | 2-3 years | 5-6 years | 6-8 years | 8+ years | EM docs leave fastest; other specs stay |
| Burnout Rate | 78% experience severe burnout within 2 years | 45% within 3 years | 32% within 4 years | 15% within 5 years | EM burnout 2x higher than Surgery |
| Monthly Violence Incidents Per 100 Doctors | 6-8 incidents | 0.5 incidents | 0.3 incidents | 0.1 incidents | EM docs experience 60x more violence than Dermatologists |
What this means: Emergency Medicine needs to hire someone new every 2-3 years per position. Surgery needs to hire someone every 5-6 years. Other specialties hire once and keep the doctor for 8+ years. EM retention is 3x worse, forcing constant recruitment. Job applicants per position shows the reality: EM can't attract talent through competition; it fills by default. EM hospitals are so desperate that they hire immediately ("You're qualified? Start Monday."). Other hospitals are selective.
Q.What Is Structural Mechanism 2: Why EM Is Least Chosen (Student Logic)?
| Factor | Why It Deters Students | Impact on Choice | Market Signal |
|---|---|---|---|
| Burnout Probability | 78% experience severe burnout within 2 years vs. 15% in Dermatology | A student calculating 5-year trajectory sees 75% risk of burnout; other specs have 10-20% risk | Students avoid EM as career path (not sustainable) |
| Violence Risk | 60-70% assaulted annually; 6-8 incidents per 100 doctors per month | Student fears working in environment where violence is normalized; sees senior doctors assaulted routinely | Students avoid EM (personal safety) |
| Income Ceiling | Rs 80K-1.4L in clinic (limited); Rs 2L in private hospital; Rs 1.2L in government | EM clinic income is 5-10x lower than Dermatology (Rs 8-20L clinic income); compensation doesn't justify 72-hour shifts | Students do math: "Why work 72 hours in EM when I can work 6 hours in Dermatology and earn 3x?" |
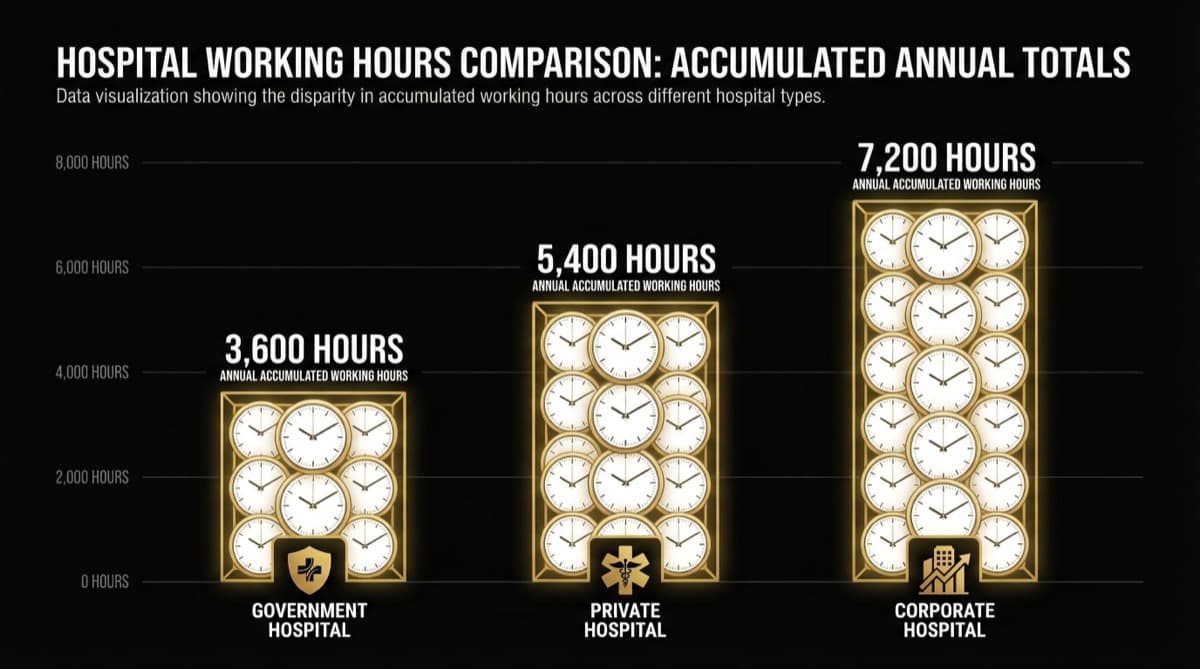
| On-Call Lifestyle | 72-hour shifts, 24-hour backup, fragmented sleep, no continuity of care | Student values life outside medicine; sees EM as "medicine owns your entire life" | Students choose specs with predictable hours (Surgery 8-10 hours/day is predictable; EM is chaos) |
| Learning Trajectory | EM is high-volume, low-continuity (see patient, stabilize, refer out, never know outcome) vs. Surgery (see patient, operate, follow-up, continuity) | Student seeks learning through patient continuity; EM offers breadth but no depth | Students avoid EM for specialized learning |
| Geographic Flexibility | EM jobs only in hospital EDs (not in clinics, not in private practice); geographically locked to hospital | Student wants geographic flexibility (start clinic, move cities, build independent practice); EM forces hospital dependence | Students see EM as career dead-end (not building personal brand/practice) |
| Post-Specialty Options | EM post-spec leads to Critical Care or EM consulting; limited diversification | Student wants options (Surgery → private practice, Derm → clinic, Cardio → interventional cathlab); EM specialized = fewer exits | Students avoid specialization without options |
Reading this: Students aren't choosing based on "I love emergency care." They're choosing based on risk-return analysis: "I want high income, low violence risk, predictable hours, independent practice, and geographic flexibility." EM fails on all five criteria. The market signal is clear: "EM is desirable only if you have no alternatives."
Q.What Is Structural Mechanism 3: Why EM Is Most Needed (Systemic Reality)?
| Why EM Is Critical | Severity | Dependency | Impact If Gap Exists |
|---|---|---|---|
| Unmet Acute Care Demand | 80% of acute care demand goes to EDs (heart attacks, strokes, poisoning, trauma, severe infections) | EDs are the only 24-hour acute care provider; no alternative infrastructure | If ED is unstaffed, acute patients die (no alternative pathway) |
| First Contact for Undiagnosed Emergencies | 40-50% of ED visits are undifferentiated emergencies (patient doesn't know what's wrong, needs rapid assessment) | ED triage + assessment = first intervention between emergency and diagnosis | If ED is unstaffed, diagnostic process collapses (no one to assess) |
| Safety Net Function | ED serves as de facto primary care (40-50% visits are non-emergency) and safety net for uninsured (40% of ED patients uninsured) | ED is only 24-hour care available to poor/uninsured; hospital can't turn away | If ED is unstaffed, poor patients have zero access to care |
| Trauma & Acute Surgery Pipeline | ED stabilizes trauma patients; without ED stabilization, trauma mortality spikes 2-3x | Trauma requires ED physician → OR team → ICU; first link is critical | If ED is unstaffed, trauma survival rates drop; surgeon work blocked (can't operate until patient stabilized) |
| Medication Overdose & Poisoning | 10-15% of ED cases are overdose/poisoning; management is time-sensitive (treatment within minutes determines survival) | ED is only 24-hour poisoning management center; antidotes require ED-level care | If ED is unstaffed, poison victims die (no antidote access) |
| Sepsis Recognition | 5-10% of ED cases are sepsis; early recognition → antibiotics within 1 hour = 40% survival; delay to 3+ hours = 20% survival | ED is first line for sepsis detection; delays are fatal | If ED is understaffed, sepsis recognition delayed; mortality spikes |
What this means: EM isn't chosen because it's hard, violent, and burns people out. But EM is needed because nobody else does what ED does (24-hour undifferentiated emergency assessment). Surgery is needed but has surplus applicants (people choose it). EM is needed but has zero applicants (people run from it). The market failure is complete: demand far exceeds supply, compensation doesn't incentivize supply, and systemic collapse is the outcome.
Need help with this?
Our team specializes in healthcare branding. Get personalized advice in a free 15-minute call.
Book a free 15-minute callQ.What Is Structural Mechanism 4: The Compensation Paradox (Why Income Doesn't Match Demand)?
| Factor | Why Compensation Is Low Despite High Demand | Economic Logic | Practical Outcome |
|---|---|---|---|
| Inelastic Demand | ED patients require care whether they can pay or not (acute, can't be deferred); hospital can't charge premium because patient has no choice | Insurance companies set price (patients covered); poor patients can't pay (uninsured); hospital can't raise fees | EM doctor's income capped by insurance rate (Rs 200-250 per consultation) regardless of demand |
| Volume-Only Economics | ED volume is high, but profit margin is low (low fee × high volume = moderate profit); hospital prioritizes ER as loss-leader (break-even) to attract inpatient admissions | Hospital budgets ED as "cost center" not "revenue center"; EM doctor salary is cost, not investment | EM doctor paid based on cost-minimization, not demand |
| No Clinic Alternative | EM doctors can't build independent clinic (emergency care isn't self-pay; patients expect hospital ED) | EM income capped at what hospital pays (Rs 2-3L monthly); can't supplement with clinic | EM compensation is single-source, low-ceiling income |
| Poor Negotiating Position | Supply shortage means hospital has to hire, but doctor has no leverage (where else will they go? only ED jobs available) | Shortage paradoxically reduces negotiating power (if doctor refuses, hospital hires next person immediately) | EM shortage = weaker bargaining position (more supply = fewer jobs = doctors compete on price) |
| Hospital Margin Pressure | Hospital faces margin pressure (insurance reimbursement low, uninsured patients uncompensated); cuts costs in low-margin ER | Hospital prioritizes profits in high-margin units (ICU, OR, specialty); ER is minimal-cost operation | EM doctor salary sacrificed to hospital margin goals |
Reading this: The paradox is real: highest demand + lowest supply = lowest compensation. Why? Because demand is inelastic (patients need it regardless) + no alternative revenue model (no clinic, no self-pay). Supply shortage doesn't translate to higher wages because hospital's margin pressure overrides. EM doctor is trapped: high demand = guaranteed job, guaranteed job = no negotiating power, no negotiating power = low compensation.
Frequently Asked Questions
Q: Will EM compensation ever improve?
A: Only if hospitals face severe EM staffing crisis (EDs close down, patients diverted, hospital loses revenue). At that point, hospital raises compensation to recruit. We're not at crisis point yet (EDs are running with critical understaffing but still functioning). Once an ED actually shuts down due to lack of doctors, compensation will spike. Expect this 3-5 years from now as burnout accelerates.
Q: Should I choose EM if I want guaranteed income?
A: Yes, EM is the only specialty with guaranteed perpetual employment (72% vacancy = always hiring). If you want income certainty (job security > income level), EM is structurally secure. Downside: compensation stagnant, violence normalized, burnout expected. If you want both income AND stability, EM is not optimal. Other specialties (Anesthesia, Critical Care) have moderate vacancy (35-50%) AND better compensation.
Q: Why doesn't the government mandate EM staffing ratios?
A: Government policy assumes market forces will balance supply and demand. Supply shortage doesn't trigger policy intervention; it triggers hospital to hire cheaper doctors or use locums. Policy intervention (mandate 2 doctors per ED shift) would require hospital compliance (no enforcement mechanism) and government funding (no budget allocated). Until policy mandates + budgets ED staffing, shortage persists and compensation remains depressed.
Q: Can EM doctors earn high income through advisory/consulting?
A: Partially. EM doctors can earn from healthtech advisory (Rs 1-2L monthly if they have 3-4 advisory roles), expert witness work (Rs 50-150K per case), and emergency medicine content creation. But these are side income, not primary. To reach Rs 15-20L monthly (comparable to Surgery), EM doctor needs: Rs 2-3L from hospital job + Rs 2-3L from consulting + Rs 1-2L from content + Rs 2L from advisory + Rs 5-8L from independent clinic or startup. It requires 3-4 income streams. Surgery doctor reaches Rs 15-20L from clinic + hospital alone. The EM advantage (guaranteed employment) is a disadvantage (forces hospital dependence, limits independent income).
futurise. builds premium healthcare brands in 48 hours. Learn more at futurise.studio