Starting salaries for MBBS doctors in Indian private hospitals have remained at Rs 40,000-60,000/month for nearly a decade — despite inflation, GDP growth, and a 40% increase in healthcare revenue over the same period. The reason is structural: MBBS seat expansion from 49,000 to 1,18,000 (a 140% increase) flooded the supply side, while demand-side consolidation created fewer, larger hospital employers with more hiring power. When 1,18,000 graduates compete for positions at a shrinking number of employers who increasingly operate as PE-backed chains optimizing for EBITDA, starting salaries don't move.
What Do the Numbers Show About a Decade of Salary Stagnation?
The data reveals a clear pattern of real wage decline. 2015 | Rs 40,000-60,000/month | Baseline | Rs 40,000-60,000 2018 | Rs 40,000-65,000/month | ~15% inflation | Rs 35,000-57,000 2021 | Rs 40,000-70,000/month | ~30% inflation | Rs 31,000-54,000 2024 | Rs 40,000-80,000/month | ~45% inflation | Rs 28,000-55,000 2026 | Rs 40,000-90,000/month | ~55% inflation | Rs 26,000-58,000
In real terms, doctors are earning less. The nominal salary may have crept up slightly at the top end, but adjusted for inflation, a doctor starting in 2026 has less purchasing power than one who started in 2015.
For comparison: entry-level IT salaries went from Rs 3-4 LPA in 2015 to Rs 5-10 LPA in 2026. MBA starting salaries grew from Rs 8-15 LPA to Rs 10-35 LPA. Doctor starting salaries remained flat.
How Has the Supply-Side Flood of Graduates Affected Salaries?
The single most important structural driver of frozen salaries is the dramatic expansion of medical seats without corresponding demand expansion.
2014 | ~49,000 | ~381 | ~45,000 2018 | ~72,000 | ~529 | ~65,000 2022 | ~97,000 | ~660 | ~90,000 2026 | ~1,18,000 | ~780+ | ~1,10,000
The mechanism: When the supply of MBBS doctors increases by 140% over a decade, and the number of hospital positions doesn't grow at the same rate, the power shifts to employers. Hospitals can offer Rs 50,000/month because there are 50 qualified applicants for every position.
This isn't a market failure — it's basic supply-demand economics. The government expanded medical seats to address the doctor shortage (a valid policy goal) without addressing the structural factors that determine where doctors work and what they earn (a policy failure).
How Does the Demand-Side Monopsony Suppress Doctor Salaries?
Supply expansion alone doesn't explain frozen salaries. The demand side changed too.
Hospital consolidation created fewer, larger employers. The PE-driven M&A wave of 2022-2024 ($4.96 billion in hospital acquisitions) consolidated hiring power. When a few large chains control a significant share of hospital positions in a city, they effectively set the market rate.
This is a monopsony — a market with many sellers (doctors) but few buyers (hospitals). In a monopsony, the buyer sets the price. And PE-backed chains set the price at the minimum level needed to fill positions.
The corporate hospital hiring model:
- Post job at Rs 50-60K/month for junior doctor
- Receive 40-100 applications
- Select from qualified candidates
- No incentive to increase offer
The hospital knows that if this doctor declines, the next one won't. The surplus of graduates ensures a permanent buyer's market for junior doctor labor.
Why Don't Government Doctor Salaries Help Set a Higher Floor?
Government doctor salaries are set by pay commissions and do increase periodically. As of the 7th Pay Commission, a government medical officer earns Rs 56,100-1,77,500/month (Level 10) with allowances often bringing total compensation to Rs 80,000-1,50,000/month.
But government positions are limited and competitive. They don't set the floor for private hospital salaries because the private and government markets are partially segmented — private hospitals don't need to match government pay to attract candidates, because many graduates are willing to accept lower private hospital salaries in exchange for metro locations, perceived career growth, and clinical exposure.
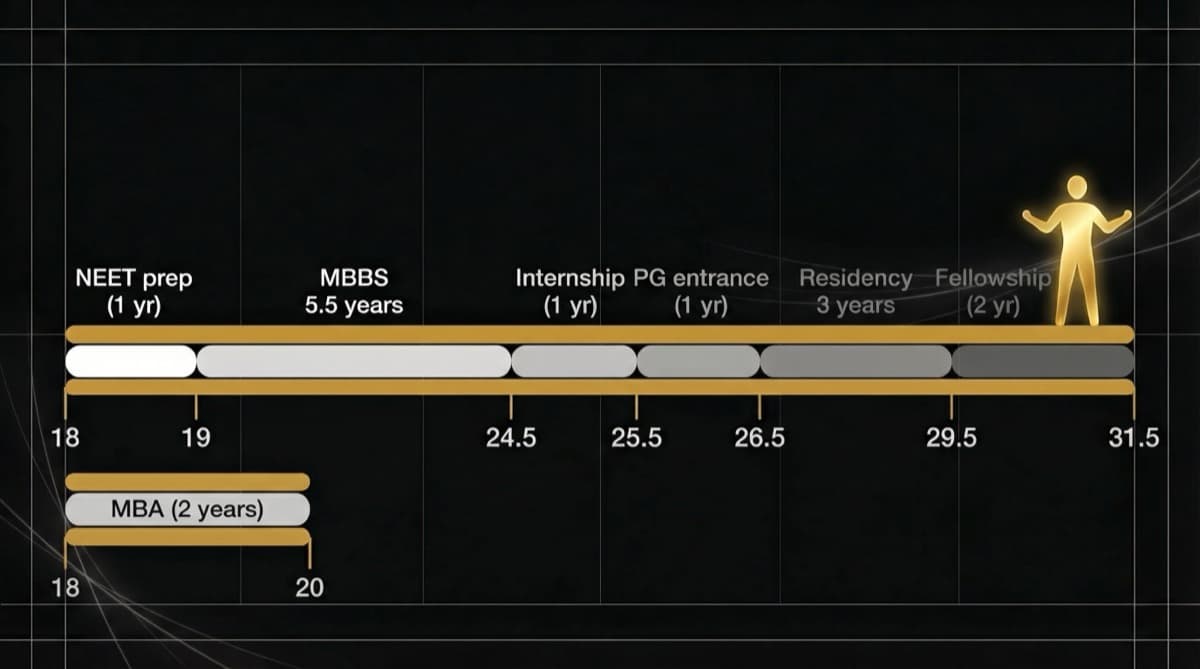
How Does the PG Bottleneck Effect Worsen Salary Stagnation?
The mismatch between MBBS output (1,18,000/year) and PG intake (~65,000/year) creates a pool of approximately 50,000+ MBBS graduates annually who cannot immediately specialize. These graduates enter the job market as generalists with limited differentiation.
What this pool does to salaries:
- 50,000+ MBBS graduates per year competing for generalist positions
- Most want to work in metros (competition intensifies in cities)
- Many are willing to accept low salaries as "temporary" while preparing for NEET PG
- Hospitals know these doctors will likely leave in 1-2 years, so they invest minimally in compensation
This creates a revolving door of low-paid junior doctors that hospitals cycle through annually — there's no retention incentive, so there's no salary growth incentive.
What Would Actually Change Starting Salaries for Doctors?
Starting salaries will remain frozen until one or more structural factors change:
- 1Supply Moderation
If MBBS seat expansion slows or stabilizes, the supply-demand imbalance gradually corrects. However, the current political incentive favors seat expansion (more colleges = more votes), so this is unlikely.
- 1Demand Expansion
If India's healthcare spending increases from 2.1% to 4-5% of GDP, more hospitals and clinics open, more positions are created, and employers compete for doctors rather than the reverse. This is possible but requires massive policy commitment.
- 1Minimum Wage Legislation
If the government mandates minimum compensation for medical professionals (similar to what exists for government doctors via pay commissions), private hospital starting salaries would need to rise. No such legislation currently exists or is proposed.
- 1Collective Bargaining
If doctors organized effectively for collective bargaining (through IMA or state associations), they could exert upward pressure on starting salaries. Cultural resistance to "unions" in medicine and legal restrictions on strikes limit this pathway.
- 1Alternative Career Paths
If a meaningful number of MBBS graduates exit clinical practice for better-paying alternatives (health-tech, pharma, consulting), the clinical supply decreases and salary pressure eases. This is slowly happening but not at scale.
Frequently Asked Questions
Why haven't doctor salaries increased with inflation? Because the supply of MBBS graduates (1,18,000/year) has grown faster than hospital demand for junior doctors. In a market with persistent oversupply, employers have no incentive to increase wages. Inflation affects what doctors pay for goods and services, but not what hospitals pay for doctors.
Are government doctor salaries better? Yes, on average. A government medical officer under the 7th Pay Commission earns Rs 80,000-1,50,000/month (including allowances) — significantly more than private hospital starting salaries. Government also offers pension, job security, and regular increments. The trade-off: limited positions, rural postings, and less clinical autonomy in some settings.
Will AI further depress doctor salaries? AI is more likely to restructure doctor roles than directly reduce salaries. Radiology, pathology, and diagnostic specialties face the most disruption. The impact on starting salaries specifically is indirect — if AI reduces the number of positions needed, the supply-demand imbalance worsens and salary stagnation continues.
How do Indian doctor starting salaries compare globally? Indian MBBS starting salaries (Rs 5-10 LPA) are among the lowest in the world for qualified physicians. UK junior doctors start at £32,398 (~Rs 34 LPA). US residents start at $60,000-70,000 (~Rs 50-58 LPA). Even adjusting for purchasing power parity, Indian doctors are paid significantly less relative to their economy's capacity.
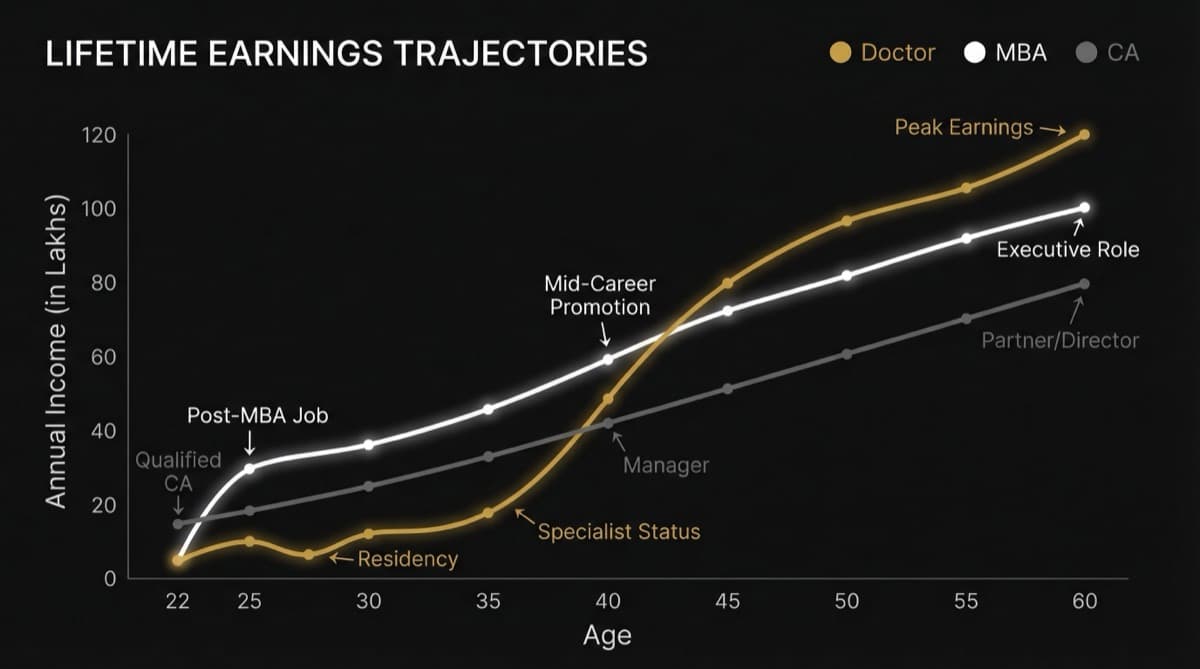
What can a fresh MBBS doctor do to earn more? Short-term: pursue positions in underserved geographies (Tier 2/3 cities, rural) where competition is lower and salaries can be 20-30% higher than metro. Medium-term: specialize — PG qualification roughly doubles to triples earning potential. Long-term: build a personal practice where you set your own fees rather than accepting hospital-determined rates.
futurise. builds premium healthcare brands in 48 hours. Learn more at futurise.studio