On this page
Rural posting pays Rs 60-80K/month while metros pay Rs 2-3L. But the real damage isn't the lower salary — it's that rural practice destroys career trajectory, forces solo medicine without backup, and becomes a financial death sentence if you try to build clinic equity. Solo practice in rural area with zero referral network, zero specialist support, and zero procedural facility is medicine at its most isolated and professionally destructive.
The Salary Structure Trap
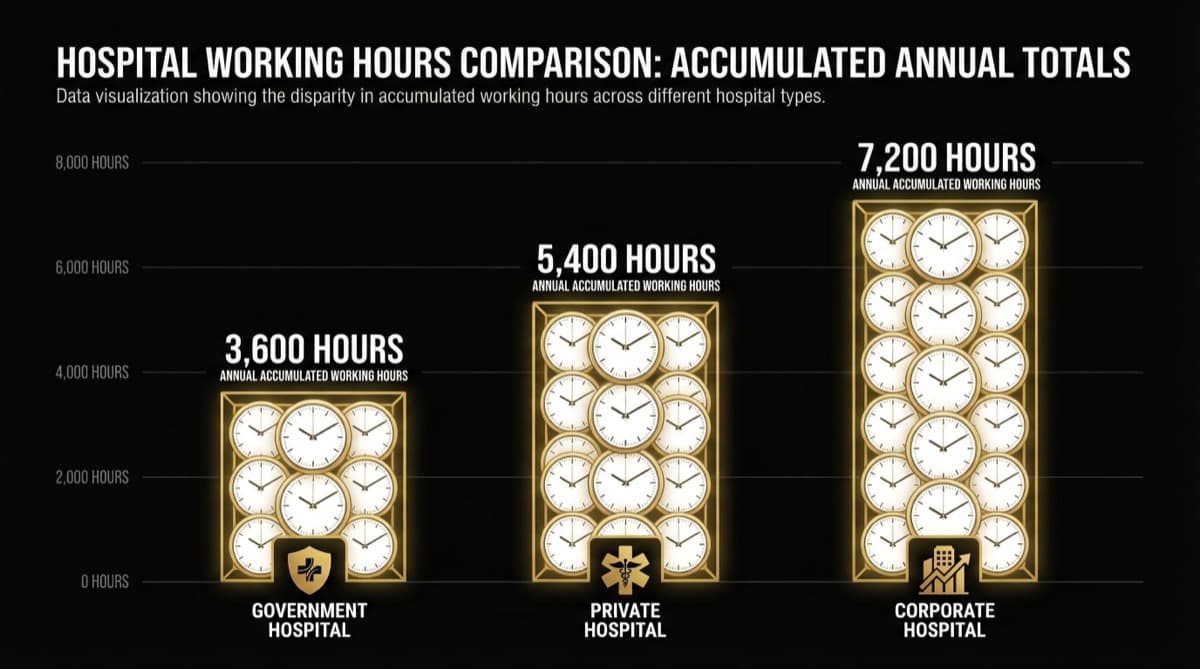
Government rural doctor (ASHA supervisor): Base Rs 40K, OPD Rs 5K, Procedures None, Total Rs 45K/month, Annual Rs 5.4L. Government CHC doctor (block level): Base Rs 55K, OPD Rs 15K, Procedures Rs 5K, Total Rs 75K, Annual Rs 9L. Government PHC doctor (village level): Base Rs 50K, OPD Rs 8K, Procedures None, Total Rs 58K, Annual Rs 7L. Private rural clinic owner: Base Rs 0, OPD Rs 15-20K, Procedures Rs 5K, Total Rs 20-25K, Annual Rs 2.4-3L.
The real income after living costs: Rural Rs 75K salary minus Rs 55K living costs = Rs 20K remaining (27% savings rate). Metro Rs 2.3L salary minus Rs 90K living costs = Rs 1.4L remaining (61% savings rate).
Over 10 years: Rs 24L saved in rural vs Rs 1.7Cr saved in metro.
Q.What Is Solo Practice Without Backup — The Professional Isolation?
In metro: Complex case — discuss with colleague. Patient needs surgery — surgeon same building. You're on leave — colleague covers. Ethical dilemma — case conference with 3 doctors. You make mistake — caught during handoff.
In rural: Complex case — decide alone. Patient needs specialist — 60-80km away (2 hours minimum). You're sick — OPD closes. Ethical dilemma — resolve yourself. You make mistake — nobody catches it.
Rural solo practice means: Full legal liability, zero institutional protection, zero peer review, zero second opinion.
Your competence ceiling in rural practice is 70%. In metro with specialist backup, it's 95%. That 25% gap compounds over career.
Q.What Is the Career Trajectory Destruction?
Metro doctor: Year 1 generalist, Year 3 developing specialty interest, Year 5 specialist recognition, Year 7 senior specialist with referral base, Year 10 recognized specialist earning Rs 5-8L/month + procedures.
Rural doctor: Year 1 generalist learning fast, Year 3 still generalist same cases, Year 5 can't develop specialty (no cases, equipment, mentors), Year 7 still generalist increasingly frustrated, Year 10 experienced generalist earning Rs 1.5-2L/month.
You can't specialize in rural area because specialty cases don't exist. You become trapped in generalist role.
Q.What Is the Clinic Ownership Death Sentence?
Rural clinic: Year 1 daily patients 3, monthly profit -Rs 5K. Year 2: 5 patients, +Rs 10K. Year 3: 8 patients, +Rs 30K. Year 4: 12 patients, +Rs 55K. Year 5: 15 patients, +Rs 75K.
You break even in year 2-3, start making money in year 4-5. But 70% of rural clinics fail in years 1-3.
Metro vs rural clinic after 10 years: Rural revenue ceiling Rs 1-1.5L/month, exit value Rs 10-20L. Metro revenue ceiling Rs 3-5L/month, exit value Rs 100L-1Cr. A metro clinic is a 10-year wealth builder. A rural clinic is a 10-year subsistence practice.
Need help with this?
Our team specializes in healthcare branding. Get personalized advice in a free 15-minute call.
Book a free 15-minute callQ.What Is The Escape Problem?
After 5 years in rural: your clinic value Rs 15-20L, selling takes 6-12 months, income during sale zero, moving costs Rs 5-10L, metro market position junior. You're financially locked in.
Frequently Asked Questions
Q: Doesn't rural posting give you "simple cases" to learn basics?
A: Yes for Year 1. After that, simple cases don't teach you complex ones. By Year 10, metro doctor is specialist; rural doctor is still a better-prepared generalist.
Q: Can't you do telemedicine to get second opinions?
A: Theoretically. Practically: Internet unreliable, consultations cost money, treating based on telemedicine has liability issues, patient still has to travel for procedures.
Q: Should young doctors do rural posting for experience?
A: 2 years government service, yes. More than 2 years is career damage. Do it for training, not career.
The actual sequence for optimal career: 1. Mandatory rural posting (2 years) — learning experience. 2. Move to tier-2/3 city (2-3 years) — transition. 3. Build clinic in tier-2 (3-5 years) — establish practice. 4. Move to metro if income/reputation allows (year 8+). Skip step 1 and do metro from start, you're Rs 1-2Cr richer by Year 10.
futurise. builds premium healthcare brands in 48 hours. Learn more at futurise.studio